Fouza Ariadni, Giagtzidis Ioakeim, Sidiropoulou Maria, Symeonidou Elissavet, Kouskoumvekaki Anna Maria, Daoudaki Maria, Petras Panagiotis, Mpallas Konstantinos
5th Surgical Department, Hippokratio General Hospital, School of Medicine, Aristotle University of Thessaloniki, Thessaloniki, 54642, Greece.
Department of Radiology, Hippokratio General Hospital, School of Medicine, Aristotle University of Thessaloniki, Thessaloniki, 54642, Greece.
Open Life Sci. 2025 Aug 5;20(1):20251127. doi: 10.1515/biol-2025-1127. eCollection 2025.
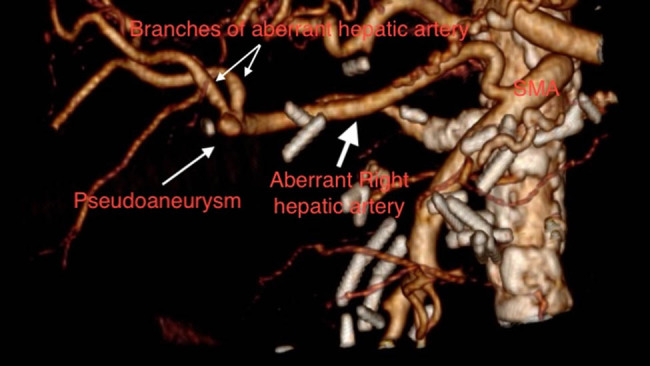
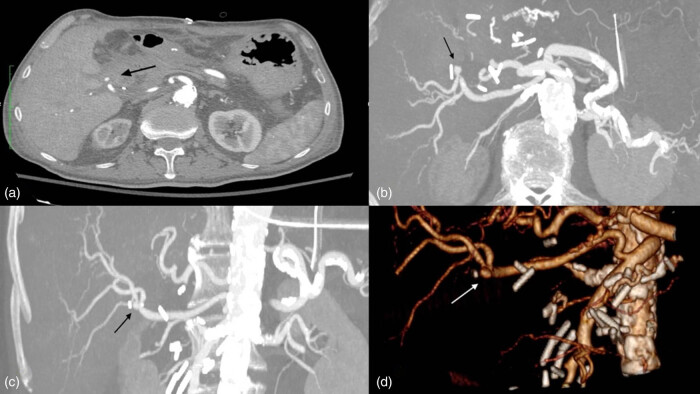
Pancreaticoduodenectomy is the standard surgical treatment for a range of malignant and some benign diseases. The mortality rate associated with this procedure has decreased to less than 3% in recent years, although the morbidity remains high at 6-40%. Common complications may include delayed gastric emptying, pancreatic fistula, intra-abdominal abscess, and gastrointestinal or intra-abdominal bleeding, among others. Bleeding and pseudoaneurysm formation are likely to be the most significant complications. This is a case report about gastrointestinal bleeding following a Whipple procedure from an aberrant hepatic artery originating from the superior mesenteric artery (SMA), treated by endovascular means. The SMA was cannulated under local anesthesia and direct puncture of the common femoral artery. Catheterization and angiogram of the aberrant right hepatic artery identified the pseudoaneurysm and bleeding site at its bifurcation. Coil embolization resulted in pseudoaneurysm occlusion and bleeding management. Hepatic perfusion was not affected as the main vasculature of the liver, namely the common hepatic artery, remained intact. The management of hemorrhage following pancreatectomy represents a significant challenge, particularly given the vulnerability of the patient cohort and the necessity for re-operation in an anatomically challenging environment. Endovascular intervention is the preferred method of treatment when applicable, as it can be performed under local anesthesia and is associated with less morbidity.
胰十二指肠切除术是一系列恶性疾病和某些良性疾病的标准外科治疗方法。近年来,该手术的死亡率已降至3%以下,尽管发病率仍高达6%-40%。常见并发症可能包括胃排空延迟、胰瘘、腹腔内脓肿以及胃肠道或腹腔内出血等。出血和假性动脉瘤形成可能是最严重的并发症。这是一例关于惠普尔手术后因起源于肠系膜上动脉(SMA)的异常肝动脉导致胃肠道出血的病例报告,通过血管内手段进行治疗。在局部麻醉下经股总动脉直接穿刺插管至SMA。对异常右肝动脉进行插管和血管造影,确定其分叉处的假性动脉瘤和出血部位。弹簧圈栓塞导致假性动脉瘤闭塞并控制了出血。由于肝脏的主要血管即肝总动脉保持完整,肝脏灌注未受影响。胰腺切除术后出血的处理是一项重大挑战,特别是考虑到患者群体的脆弱性以及在解剖结构复杂的环境中再次手术的必要性。血管内介入治疗在适用时是首选的治疗方法,因为它可以在局部麻醉下进行,且发病率较低。