Kunjok David Majuch, Mwangi John Gachohi, Kairu-Wanyoike Salome, Kinyua Johnson, Mambo Susan
Department of Environmental Health and Disease Control, School of Public Health, Jomo Kenyatta University of Agriculture and Technology, Juja, Kenya.
World Health Organization, Juba, South Sudan.
PLoS One. 2025 Aug 8;20(8):e0329984. doi: 10.1371/journal.pone.0329984. eCollection 2025.
Kenya ranks among the top 30 countries with a high tuberculosis (TB) burden globally. With a TB prevalence of 558 per 100,000, only 46% of TB cases are diagnosed and treated, leaving 54% undiagnosed and at risk of spreading the disease. This study analyzed the spatial distribution of tuberculosis diagnostic delays and their association with health care accessibility and socioeconomic inequalities in Nairobi County, Kenya.
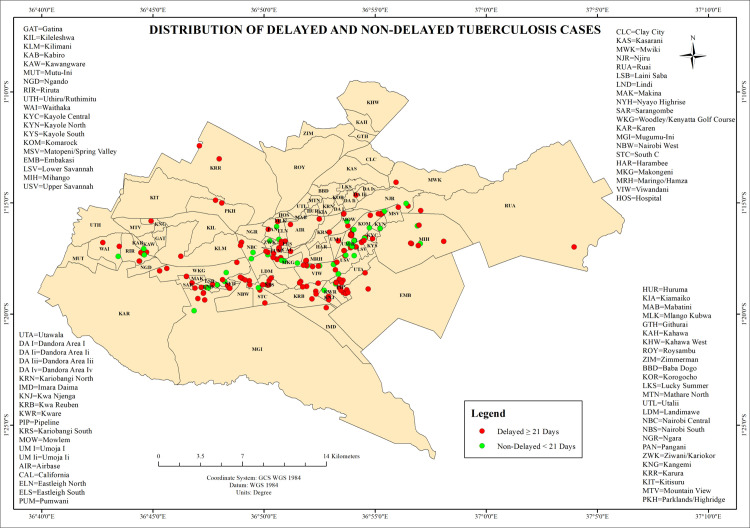
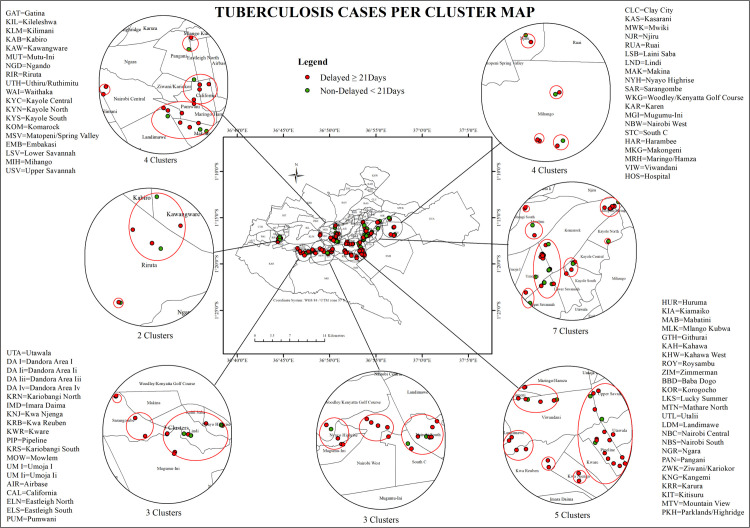
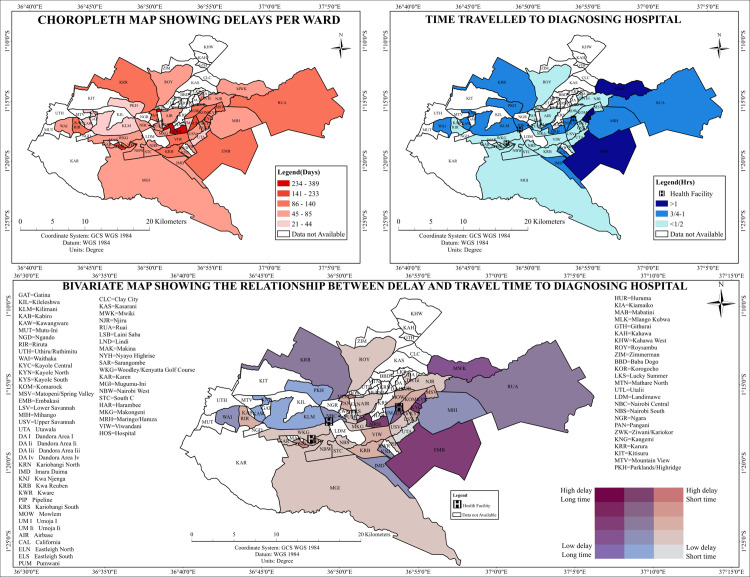
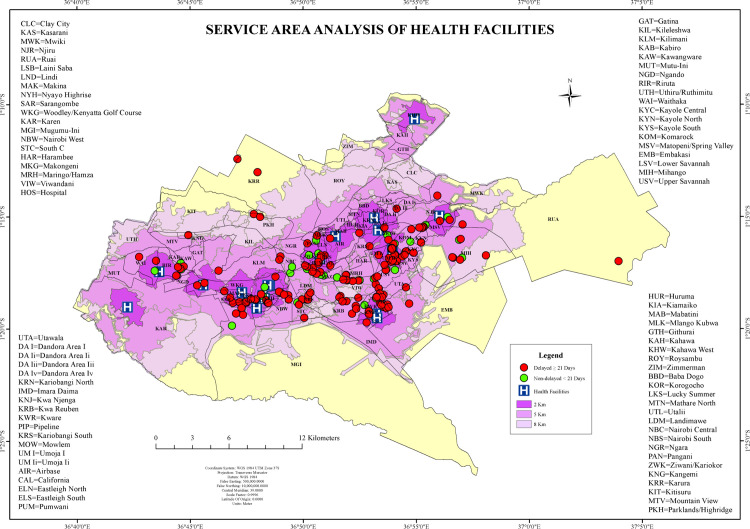
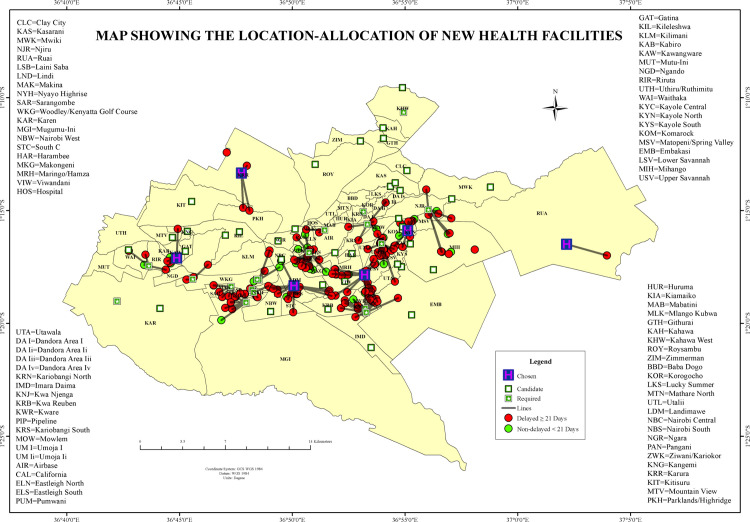
The cross-sectional study included 222 newly diagnosed bacteriologically confirmed Mycobacterium tuberculosis (Mtb) patients from Mbagathi County Hospital (MCH), Mama Lucy Kibaki Hospital (MLKH), and Rhodes Chest Clinic (RCC) in Nairobi County, Kenya. Patients were recruited consecutively through census sampling and categorized into two groups: delayed diagnosis (≥21 days from symptom onset) and non-delayed (<21 days) as defined by the WHO cutoff point. Patients' residential locations were georeferenced using handheld GPS devices and captured digitally via Kobo Collect. Spatial analyses were performed using ArcGIS Pro, version, where Global Moran's I statistic was used to assess spatial autocorrelation in the distribution of TB cases.
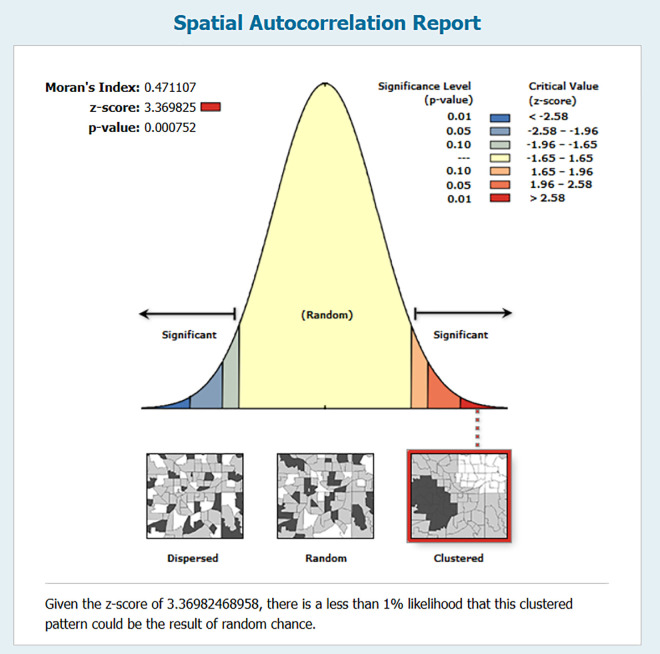
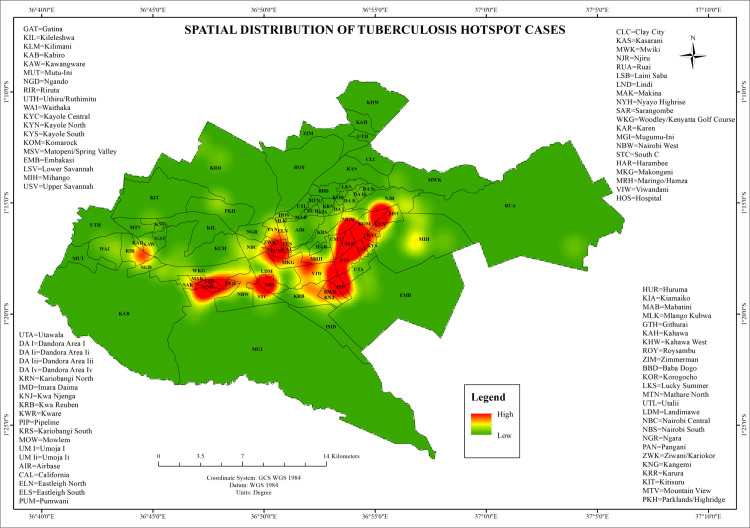
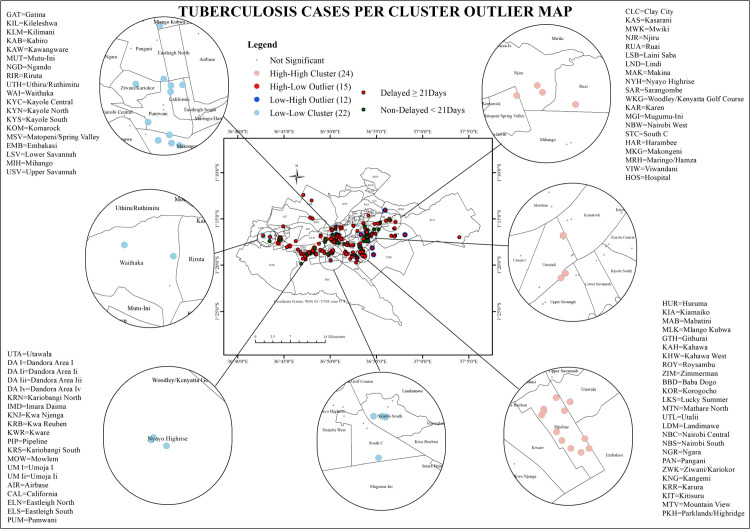
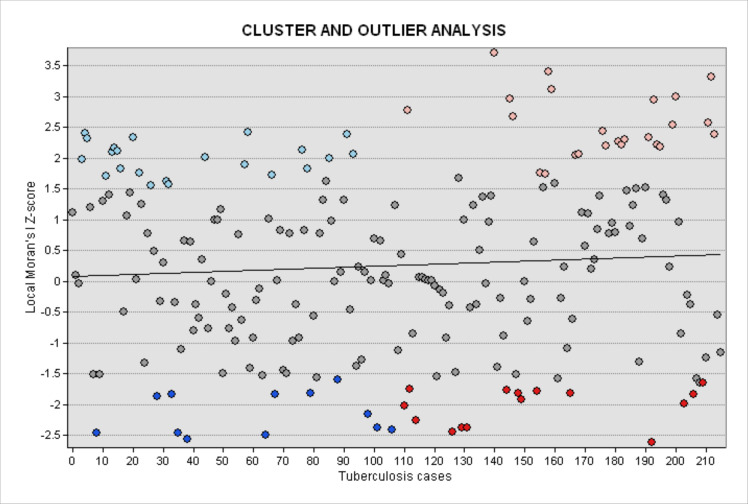
Spatial analyses identified 28 statistically significant clusters of delayed TB diagnoses within Nairobi County. Spatial autocorrelation analysis using Moran's I revealed a significant clustered distribution (Moran's Index = 0.471, z-score = 3.370, p < 0.001). Hotspot analysis with the Getis-Ord Gi* statistic detected high-delay clusters (z > 2.58, p < 0.001) in informal settlements.
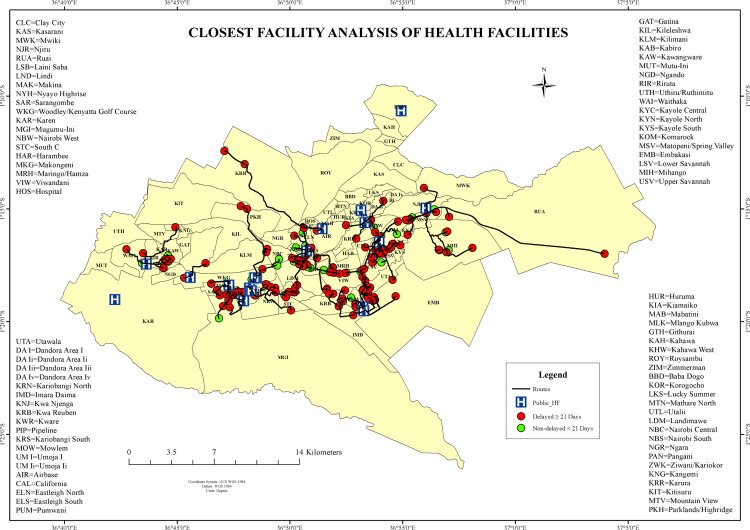
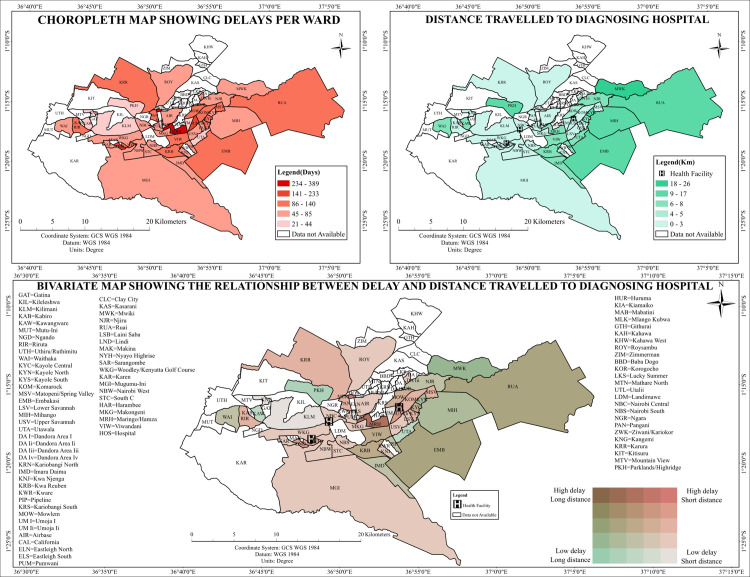
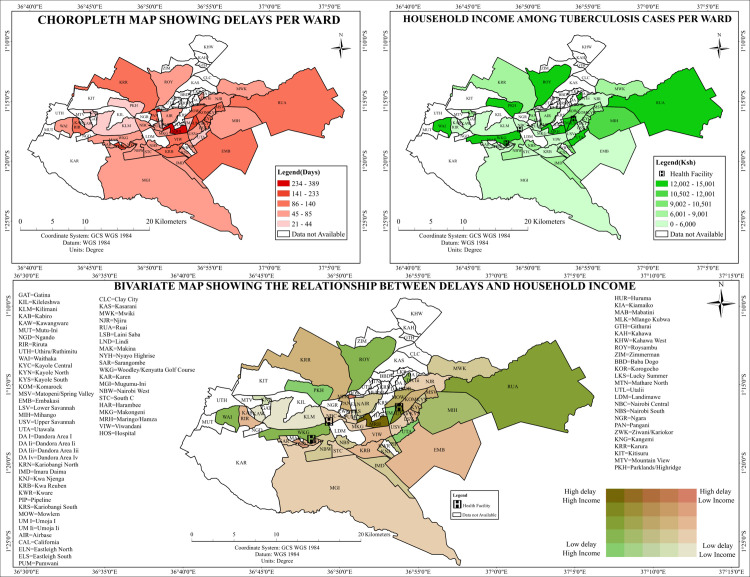
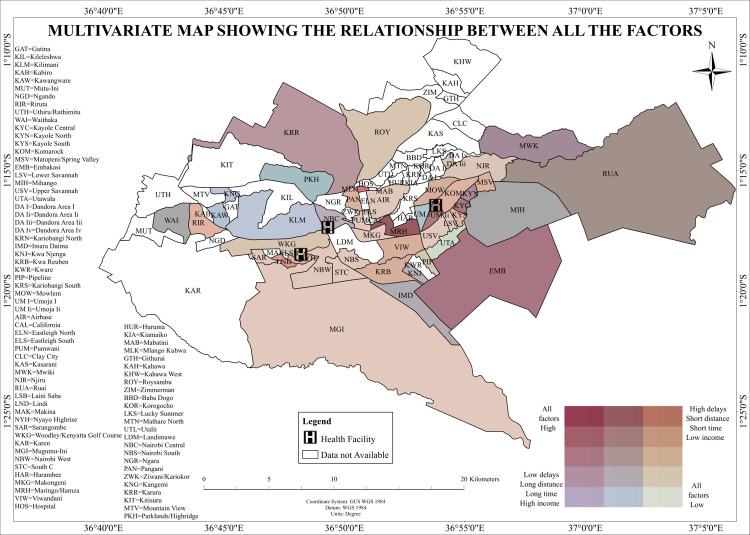
The study revealed significant spatial clustering of delayed TB diagnoses in Nairobi County, particularly in informal settlements. In contrast, timely diagnoses were predominantly clustered in high-income areas like Lang'ata and Karen. These clusters were significantly associated with lower household income and increased travel time to health facilities which underscored the need for targeted implementation of TB diagnostic services and control measures in the wards with the highest delays.
肯尼亚是全球结核病负担较高的30个国家之一。结核病患病率为每10万人中有558例,仅有46%的结核病病例得到诊断和治疗,54%的病例未被诊断,存在传播疾病的风险。本研究分析了肯尼亚内罗毕县结核病诊断延误的空间分布及其与医疗服务可及性和社会经济不平等的关联。
这项横断面研究纳入了来自肯尼亚内罗毕县姆巴加蒂县医院(MCH)、妈妈露西·基巴基医院(MLKH)和罗德胸部诊所(RCC)的222例新诊断的经细菌学确诊的结核分枝杆菌(Mtb)患者。通过普查抽样连续招募患者,并根据世界卫生组织的临界值分为两组:诊断延误(症状出现后≥21天)和未延误(<21天)。使用手持GPS设备对患者的居住地点进行地理定位,并通过Kobo Collect进行数字采集。使用ArcGIS Pro版本进行空间分析,其中全局莫兰指数I统计量用于评估结核病病例分布的空间自相关性。
空间分析在内罗毕县确定了28个具有统计学意义的结核病诊断延误聚集区。使用莫兰指数I进行的空间自相关性分析显示出显著的聚集分布(莫兰指数=0.471,z分数=3.370,p<0.001)。使用Getis-Ord Gi*统计量进行的热点分析在内罗毕的非正式定居点检测到高延误聚集区(z>2.58,p<0.001)。
该研究揭示了内罗毕县结核病诊断延误存在显著的空间聚集现象,尤其是在非正式定居点。相比之下,及时诊断主要集中在诸如兰加塔和卡伦等高收入地区。这些聚集区与较低的家庭收入和前往医疗机构的时间增加显著相关,这突出表明需要在延误率最高的病房有针对性地实施结核病诊断服务和控制措施。