Li Xing, Sun Qing, Shao Long, Zhu Zhihui, Zhao Ruiqi, Meng Fanhao, Zhao Zehua, Jihu Kedi, Xiang Xiting, Fu Tianyu, Ai Danni, Huo Minghao, Wang Xiaojun, Yang Jian, Zhang Tao
Division of Maxillofacial Surgery, Department of Stomatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Department of Plastic and Reconstructive Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
BMC Oral Health. 2025 Aug 9;25(1):1309. doi: 10.1186/s12903-025-06566-2.
Oral and maxillofacial tumors, particularly those requiring mandibular reconstruction, present significant clinical challenges due to the complexities involved in achieving precise surgical outcomes and ensuring post-operative stability. Traditional methods for mandibular reconstruction, such as freehand bending of titanium plates, often result in errors in osteotomy and reconstruction, compromising both the precision and stability of the procedure.
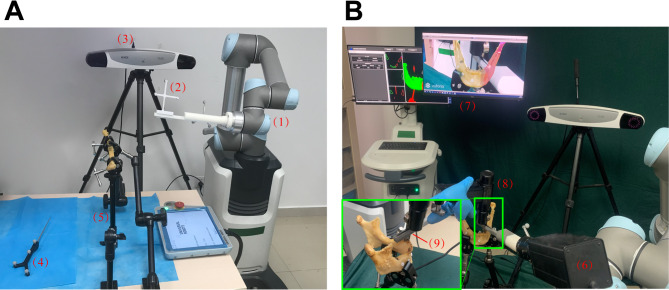
This study initially developed the Robot-assisted Augmented Reality Osteotomy Navigation System (RARONS) and constructed a virtual surgical plan using imaging data. In this robot-assisted cadaveric osteotomy study, 20 Non-Flap Fibulas (NFFs) and 9 Free Flap Fibulas (FFFs) were included to evaluate the impact of pedicle factors on osteotomy precision. Augmented Reality technology enabled surgeons to intuitively perform procedures according to the virtual plan during the robot-assisted osteotomy process. Additionally, in the mandibular reconstruction experiments using cadavers, 11 NFFs and 9 FFFs were included to assess the influence of pedicle factors on reconstruction accuracy. 11 fibulas were reconstructed using surgical guide-plate methods, while 9 fibulas were reconstructed using freehand methods to evaluate the impact of surgical guide plates on reconstruction precision. Finally, an evaluation framework was established to quantify the precision of osteotomy and reconstruction, with osteotomy errors measured in terms of length, angle, and volume, and mandibular reconstruction errors assessed based on width, height, anteroposterior diameter, and symmetry.
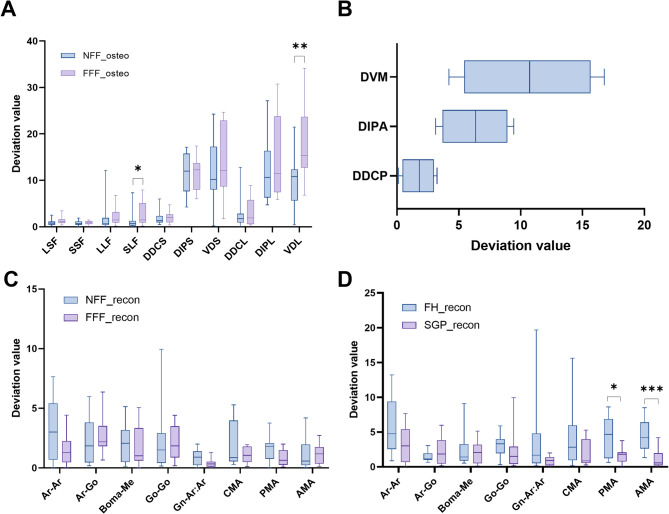
In the osteotomy experiments, the Non-Flap Fibula group demonstrated higher accuracy compared to the Free Flap Fibula group, with mean errors in osteotomy length, angle, and volume recorded as 1.08 ± 1.57 mm, 11.78° ± 5.72°, and 10.76 ± 5.94%, respectively. Similarly, in the mandibular osteotomy experiment, the errors in osteotomy length were within clinically acceptable ranges, with mean errors in length, angle, and volume reported as 1.75 ± 1.32 mm, 6.32° ± 2.71°, and 10.61 ± 5.29%, respectively. In the reconstruction experiments, the presence of a pedicle fibula did not significantly affect the error rate in mandibular reconstruction. Additionally, the personalized surgical guide-plate reconstruction group showed superior accuracy in width, anteroposterior diameter, and symmetry compared to the traditional freehand reconstruction group. The posterior mandibular angle and anterior mandibular angle for the personalized group were 1.57° ± 1.07° and 1.16° ± 1.31°, respectively.
This study demonstrated that RARONS significantly improved osteotomy accuracy and enhanced mandibular reconstruction precision using personalized pseudo-titanium plates and guide-plates. These advancements lay the foundation for integrating digital osteotomy navigation and personalized surgical guide-plate technology into clinical maxillofacial surgery.
口腔颌面部肿瘤,尤其是那些需要下颌骨重建的肿瘤,由于实现精确手术结果和确保术后稳定性所涉及的复杂性,带来了重大的临床挑战。传统的下颌骨重建方法,如钛板的徒手弯曲,常常导致截骨术和重建中的误差,损害了手术的精度和稳定性。
本研究最初开发了机器人辅助增强现实截骨导航系统(RARONS),并使用成像数据构建了虚拟手术计划。在这项机器人辅助的尸体截骨术研究中,纳入了20根非带蒂腓骨(NFFs)和9根游离皮瓣腓骨(FFFs),以评估蒂因素对截骨精度的影响。增强现实技术使外科医生能够在机器人辅助截骨过程中根据虚拟计划直观地进行手术。此外,在使用尸体的下颌骨重建实验中,纳入了11根NFFs和9根FFFs,以评估蒂因素对重建准确性的影响。11根腓骨采用手术导板方法进行重建,而9根腓骨采用徒手方法进行重建,以评估手术导板对重建精度的影响。最后,建立了一个评估框架来量化截骨术和重建的精度,截骨误差以长度、角度和体积来衡量,下颌骨重建误差根据宽度、高度、前后径和对称性来评估。
在截骨术实验中,非带蒂腓骨组的准确性高于游离皮瓣腓骨组,截骨长度、角度和体积的平均误差分别记录为1.08±1.57毫米、11.78°±5.72°和10.76±5.94%。同样,在下颌骨截骨术实验中,截骨长度误差在临床可接受范围内,长度、角度和体积的平均误差分别报告为1.75±1.32毫米、6.32°±2.71°和10.61±5.29%。在重建实验中,带蒂腓骨的存在对下颌骨重建的误差率没有显著影响。此外,个性化手术导板重建组在宽度、前后径和对称性方面的准确性优于传统徒手重建组。个性化组的下颌骨后角和前角分别为1.57°±1.07°和1.16°±1.31°。
本研究表明,RARONS使用个性化的假钛板和导板显著提高了截骨准确性,并增强了下颌骨重建精度。这些进展为将数字截骨导航和个性化手术导板技术整合到临床颌面外科奠定了基础。