Kirkham Aidan M, Paquet Maude, Fergusson Dean A, Graham Ian D, Presseau Justin, McIsaac Daniel I, Nagpal Sudhir K, de Launay David, Abdul Sami Aftab, Shorr Risa, Grimshaw Jeremy M, Roberts Derek J
Division of Vascular and Endovascular Surgery, Department of Surgery, University of Ottawa, Ottawa, Ontario, Canada.
School of Epidemiology and Public Health, Faculty of Medicine, University of Ottawa, Ottawa, Ontario, Canada.
EClinicalMedicine. 2025 Jul 31;86:103391. doi: 10.1016/j.eclinm.2025.103391. eCollection 2025 Aug.
Guidelines recommend that adults with peripheral artery disease (PAD) take antiplatelets, statins, and antihypertensives. However, it is unclear how frequently clinicians do not prescribe these medications (ie, underprescription), how often patients fail to fill/refill their prescriptions (ie, nonadherence), which factors increase underprescription/nonadherence risk, and whether underprescription/nonadherence are associated with outcomes.
We searched MEDLINE, EMBASE, CENTRAL, and Evidence-Based Medicine Reviews (January 1, 2006-to-February 18th, 2025) for studies reporting cumulative incidences/point prevalences of clinician underprescription and/or patient nonadherence to antiplatelets, statins, and/or antihypertensives; adjusted-risk factors for underprescription/nonadherence; and adjusted-outcomes associated with underprescription/nonadherence among adults with PAD. Two investigators independently screened citations, extracted data, and assessed risk of bias. Data were pooled using random-effects models. Estimate certainty was communicated using GRADE. The study was registered on PROSPERO (CRD42022362801).
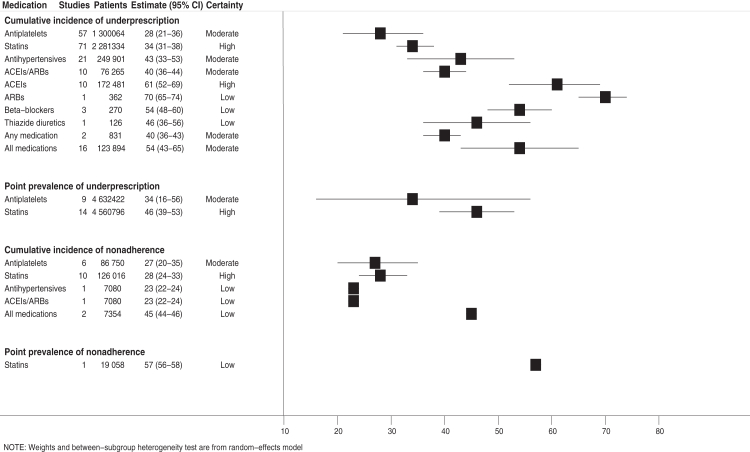
Among 4206 citations identified, 125 studies (n = 14,681,801 participants; 37% female) were included. The pooled cumulative incidence of antiplatelet, statin, and antihypertensive (among those with PAD and hypertension) underprescription was 28% (95% confidence interval [CI] = 21-36%; moderate-certainty), 34% (95% CI = 31-38%; high-certainty), and 43% (95% CI = 33-53%; moderate-certainty), respectively. The cumulative incidence of antiplatelet, statin, and antihypertensive nonadherence was 27% (95% CI = 20-35%; moderate-certainty), 28% (95% CI = 24-33%; high-certainty), and 23% (95% CI = 22-24%; low-certainty), respectively. Underprescription was more common in population-based studies and those enrolling more females and past/current smokers while nonadherence was more common in studies enrolling more patients with diabetes. Underprescription risk factors included female sex, advanced age, malignancy history, and chronic limb-threatening ischemia (all moderate-certainty). Nonadherence risk factors included advanced age, comorbidity burden, and receiving specialist mental health care (all moderate-certainty). Underprescription was associated with increased major adverse cardiac events, all-cause mortality, and decreased amputation-free time (all moderate-certainty).
One-quarter-to-one-half of adults with PAD are not prescribed antiplatelets, statins, and antihypertensives. Further, approximately one-quarter of these patients do not adhere to these medications after prescription.
This research was supported by a 2024 Vanier Canada Graduate Scholarship (awarded to AMK and supervised by DJR), a Graham Farquharson Physician Services Incorporated Knowledge Translation Fellowship (awarded to DJR), and a Research Program Award, University of OttawaDepartment of Surgery Annual Competition (awarded to DJR).
指南建议患有外周动脉疾病(PAD)的成年人服用抗血小板药物、他汀类药物和抗高血压药物。然而,目前尚不清楚临床医生不开具这些药物处方的频率(即处方不足)、患者不取药/不续方的频率(即不依从)、哪些因素会增加处方不足/不依从的风险,以及处方不足/不依从是否与预后相关。
我们检索了MEDLINE、EMBASE、CENTRAL和循证医学综述(2006年1月1日至2025年2月18日),以查找报告临床医生处方不足和/或患者不依从抗血小板药物、他汀类药物和/或抗高血压药物的累积发病率/点患病率;处方不足/不依从的调整风险因素;以及与PAD成人患者处方不足/不依从相关的调整后结局的研究。两名研究人员独立筛选文献、提取数据并评估偏倚风险。使用随机效应模型汇总数据。使用GRADE传达估计的确定性。该研究已在PROSPERO(CRD42022362801)上注册。
在识别出的4206篇文献中,纳入了125项研究(n = 14,681,801名参与者;37%为女性)。抗血小板药物、他汀类药物和抗高血压药物(在患有PAD和高血压的患者中)处方不足的汇总累积发病率分别为28%(95%置信区间[CI] = 21 - 36%;中等确定性)、34%(95% CI = 31 - 38%;高确定性)和43%(95% CI = 33 - 53%;中等确定性)。抗血小板药物、他汀类药物和抗高血压药物不依从的累积发病率分别为27%(95% CI = 20 - 35%;中等确定性)、28%(95% CI = 24 - 33%;高确定性)和23%(95% CI = 22 - 24%;低确定性)。处方不足在基于人群的研究以及纳入更多女性和既往/当前吸烟者的研究中更为常见,而不依从在纳入更多糖尿病患者的研究中更为常见。处方不足的风险因素包括女性、高龄、恶性肿瘤病史和慢性肢体威胁性缺血(均为中等确定性)。不依从的风险因素包括高龄、合并症负担和接受专科心理健康护理(均为中等确定性)。处方不足与主要不良心脏事件增加、全因死亡率增加以及无截肢时间缩短相关(均为中等确定性)。
四分之一至二分之一的PAD成年患者未被开具抗血小板药物、他汀类药物和抗高血压药物。此外,这些患者中约有四分之一在处方后不依从这些药物治疗。
本研究得到了2024年加拿大瓦尼尔研究生奖学金(授予AMK,由DJR指导)、格雷厄姆·法夸尔森医师服务公司知识转化奖学金(授予DJR)以及渥太华大学外科系年度竞赛研究项目奖(授予DJR)的支持。