Braffett Barbara H, El Ghormli Laure, Martin Catherine, White Neil H, Hirsch Irl B, Bantle Anne, Carlson Anders, Leschek Ellen, Gubitosi-Klug Rose, Soliman Elsayed Z, Vella Adrian, Perkins Bruce A, Bebu Ionut, Pop-Busui Rodica
The Biostatistics Center, George Washington University, 6110 Executive Blvd, Suite 750, Rockville, MD, 20852, USA.
Department of Internal Medicine, Division of Metabolism, Endocrinology, and Diabetes, University of Michigan, Ann Arbor, MI, USA.
Cardiovasc Diabetol. 2025 Aug 13;24(1):334. doi: 10.1186/s12933-025-02856-9.
To describe longitudinal prevalence and risk factors associated with cardiovascular autonomic neuropathy (CAN), defined by heart rate variability (HRV) indices, and evaluate the impact of CAN on cardiovascular disease (CVD), in adults with type 1 diabetes (T1D) from the Epidemiology of Diabetes Interventions and Complications (EDIC) study.
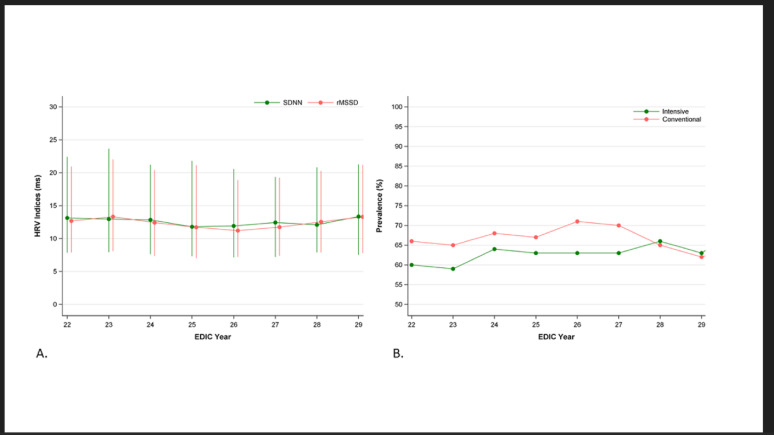
Standard resting electrocardiogram (ECG) recordings were obtained annually in 997 participants (mean ± SD age 56.2 ± 6.8 years; T1D duration 34.7 ± 7.9 years; 48% female) between 2015 and 2022. The standard deviation of normally conducted R-R intervals (SDNN) and root mean square of successive differences between normal-to-normal R-R intervals (rMSSD) were used to define CAN using previously validated cut-offs in this cohort from gold-standard cardiovascular reflex tests (CARTs). Generalized estimating equation models were used to evaluate the association of ECG-derived CAN with individual risk factors over repeated time points. Kaplan-Meier estimates were used to describe the cumulative incidence of the first occurrence of any-CVD and of MACE by ECG-derived CAN status, and Cox proportional hazards regression models were used to estimate the effect of ECG-derived CAN adjusted for age and HbA1c.
The prevalence of ECG-derived CAN (~ 64%) was stable. Higher pulse rate (OR [95% CI] 1.08 [1.07,1.10] per 1 bpm) and HbA1c (1.43 [1.29,1.58] per 1%) were the most significant risk factors for CAN, followed by older age, male sex, higher albumin excretion rate, and hypertension history. The cumulative incidence of first occurrence of any-CVD over 7 years of follow-up was significantly higher in participants with vs. without CAN (HR [95% CI] any-CVD 2.37 [1.43,3.94]), which remained significant adjusting for mean HbA1c and age, but was attenuated with further adjustment for other factors.
The prevalence of and risk factors for standard resting ECG-derived CAN were similar to previously reported estimates from CARTs. CVD risk was significantly higher in those with vs. without CAN. These data support future studies examining the diagnostic utility of HRV indices at the point of care for risk stratification.
clinicaltrials.gov NCT00360815 and NCT00360893.
在糖尿病干预与并发症流行病学(EDIC)研究中,描述1型糖尿病(T1D)成年患者中心血管自主神经病变(CAN)的纵向患病率及与心率变异性(HRV)指标相关的危险因素,并评估CAN对心血管疾病(CVD)的影响。
在2015年至2022年期间,每年对997名参与者(平均年龄±标准差56.2±6.8岁;T1D病程34.7±7.9年;48%为女性)进行标准静息心电图(ECG)记录。采用正常传导的R-R间期标准差(SDNN)和正常R-R间期连续差值的均方根(rMSSD),根据该队列先前经金标准心血管反射试验(CARTs)验证的临界值来定义CAN。使用广义估计方程模型评估重复时间点上ECG衍生的CAN与个体危险因素之间的关联。采用Kaplan-Meier估计法描述根据ECG衍生的CAN状态首次发生任何CVD和主要不良心血管事件(MACE)的累积发生率,并使用Cox比例风险回归模型估计经年龄和糖化血红蛋白(HbA1c)调整后的ECG衍生的CAN效应。
ECG衍生的CAN患病率(约64%)稳定。较高的脉搏率(每1次心跳每分钟的比值比[95%置信区间]1.08[1.07,1.10])和HbA1c(每1%为1.43[1.29,1.58])是CAN最显著的危险因素,其次是年龄较大、男性、较高的白蛋白排泄率和高血压病史。在随访7年期间,有CAN与无CAN的参与者首次发生任何CVD的累积发生率显著更高(任何CVD的风险比[95%置信区间]为2.37[1.43,3.94]),在调整平均HbA1c和年龄后仍显著,但在进一步调整其他因素后减弱。
标准静息ECG衍生的CAN的患病率和危险因素与先前CARTs报告的估计值相似。有CAN者的CVD风险显著高于无CAN者。这些数据支持未来研究在医疗点检查HRV指标对风险分层的诊断效用。
clinicaltrials.gov NCT00360815和NCT00360893。