Gül Oğuz, Erdivanlı Özlem Çelebi, Birinci Mehmet, Terzi Suat, Çeliker Metin, Okçu Oğuzhan, Öztürk Çiğdem, Yemiş Tuğba, Çeliker Fatma Beyazal, Özergin Coşkun Zerrin, Dursun Engin
Department of Otorhinolaryngology, Faculty of Medicine, Recep Tayyip Erdogan University, Rize 53200, Turkey.
Department of Pathology, Faculty of Medicine, Recep Tayyip Erdogan University, Rize 53200, Turkey.
J Clin Med. 2025 Jul 23;14(15):5224. doi: 10.3390/jcm14155224.
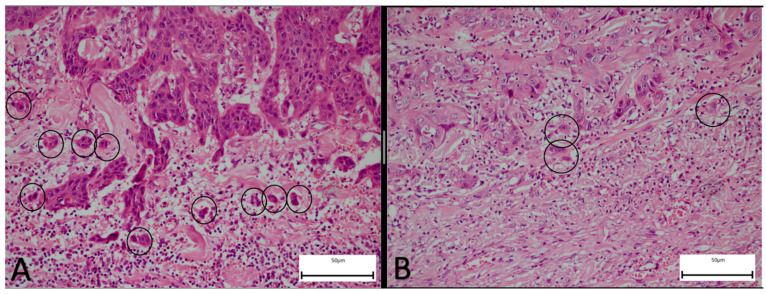
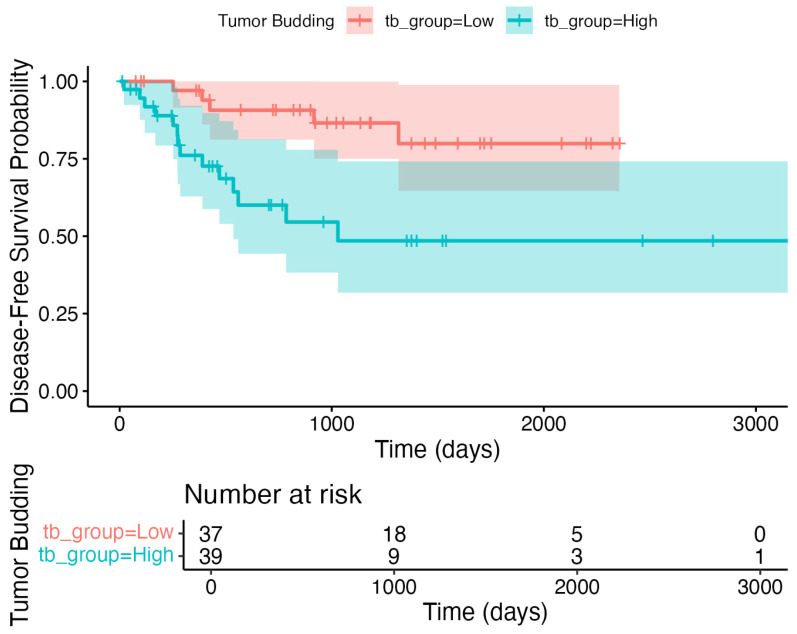
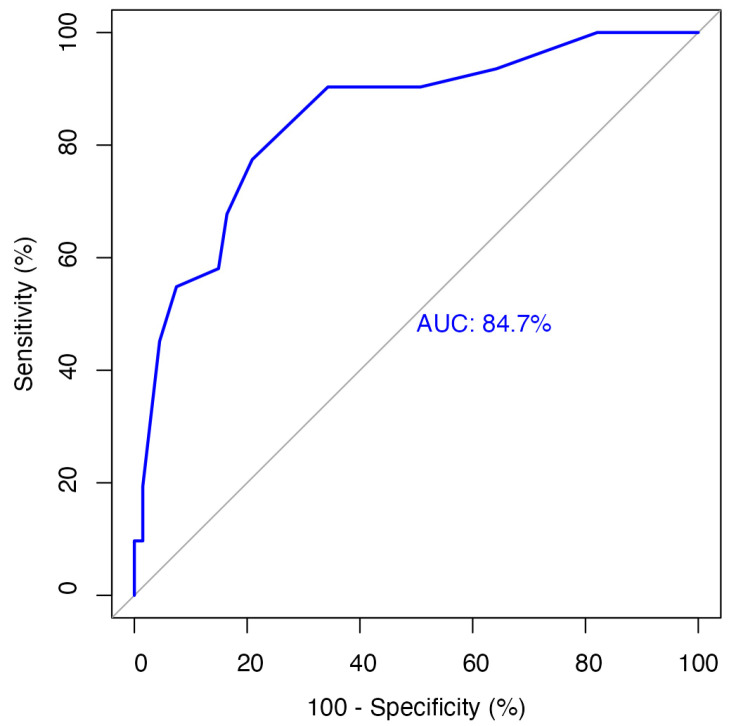
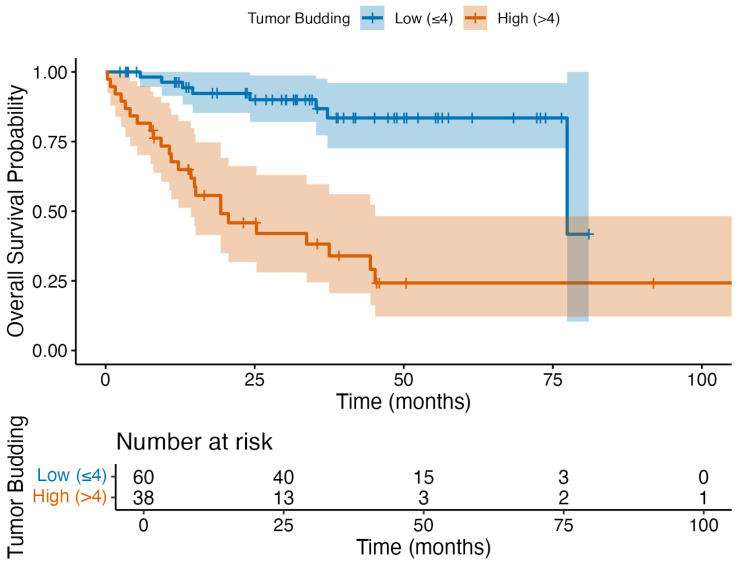
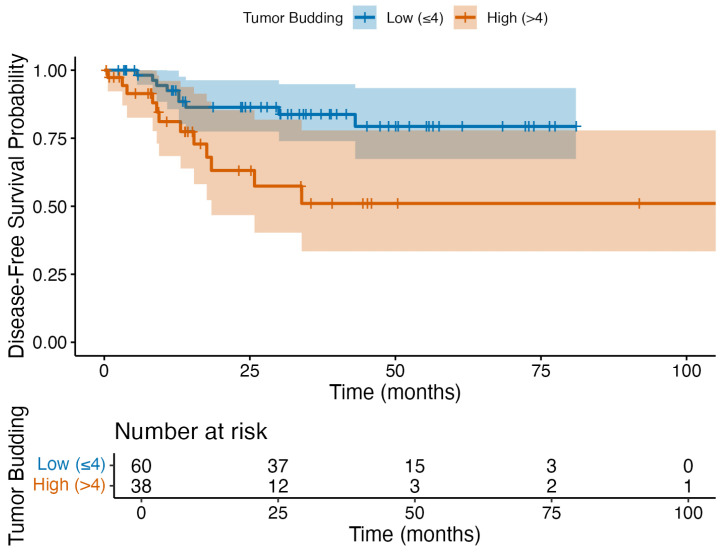
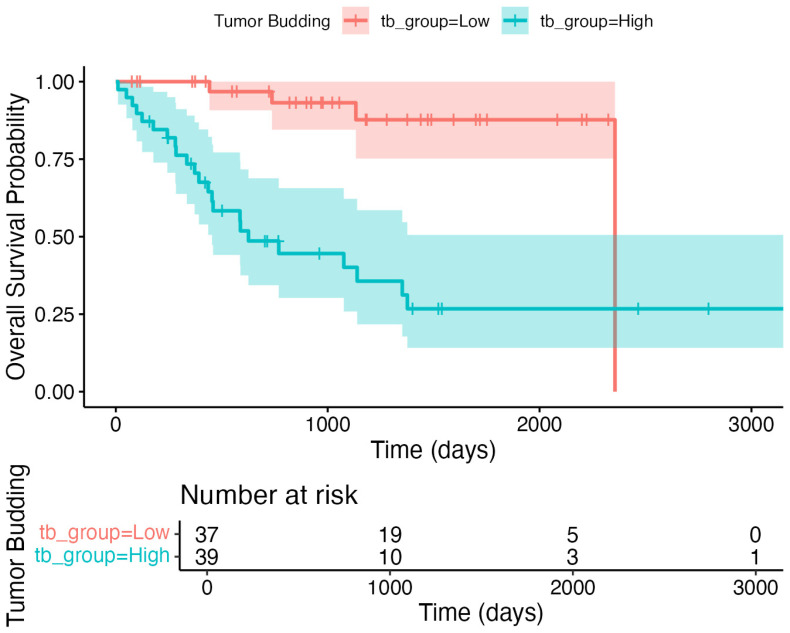
Tumor budding (TB)-clusters of one to five tumor cells at the invasive front-has emerged as a prognostic marker in various cancers. Its prognostic value in head and neck squamous cell carcinoma (HNSCC) is unclear. We retrospectively analyzed 98 HNSCC patients. The tumor buds were counted on hematoxylin-eosin-stained sections as per the 2016 International Tumor Budding Consensus Conference (ITBCC) guidelines. An optimal cutoff was determined by ROC analysis using excisional lymph nodes and five-year overall survival (OS) as the endpoint, stratifying patients into low- (≤4 buds) and high-risk (>4 buds) groups. The associations with clinicopathological features, OS, and disease-free survival (DFS) were assessed using Kaplan-Meier curves and Cox regression. Among the 98 patients (median follow-up 58 months, range 18-108), 32 (32.7%) died. The optimal TB cutoff was 4.5 (AUC 0.85, 95% CI 0.76-0.93). High TB was associated with poorer five-year OS (26.4% vs. 85.3%). Multivariate Cox regression identified TB and extranodal extension as independent predictors of OS (TB HR: 3.4, 95% CI 1.3-9.2, = 0.013). In the laryngeal cancer subgroup, TB was associated with worse survival in the univariate analysis (HR 7.5, 95% CI 1.6-35.6, = 0.011), though this was not significant in the multivariate modeling. High TB independently predicted neck lymph node metastasis (multivariate OR 4.9, 95% CI 1.2-20.5, = 0.029), which was present in 65.8% of the high-TB vs. 31.7% of the low-TB patients. High TB correlated with advanced AJCC stage and lymphovascular invasion. No clinicopathological factors, including TB, independently predicted DFS, in either the full cohort or the laryngeal subgroup. High tumor budding denotes an aggressive HNSCC phenotype and may guide decisions on elective neck dissection. Its assessment is simple, cost-effective, and potentially valuable for routine pathology, pending external validation.
肿瘤芽生(TB)——侵袭前沿处由一至五个肿瘤细胞组成的细胞簇——已成为多种癌症的预后标志物。其在头颈部鳞状细胞癌(HNSCC)中的预后价值尚不清楚。我们对98例HNSCC患者进行了回顾性分析。根据2016年国际肿瘤芽生共识会议(ITBCC)指南,在苏木精-伊红染色切片上计数肿瘤芽。以切除的淋巴结和五年总生存期(OS)为终点,通过ROC分析确定最佳截断值,将患者分为低风险(≤4个芽)和高风险(>4个芽)组。使用Kaplan-Meier曲线和Cox回归评估与临床病理特征、OS和无病生存期(DFS)的相关性。在98例患者中(中位随访58个月,范围18 - 108个月),32例(32.7%)死亡。最佳TB截断值为4.5(AUC 0.85,95% CI 0.76 - 0.93)。高TB与较差的五年OS相关(26.4%对85.3%)。多变量Cox回归确定TB和结外扩展是OS的独立预测因素(TB HR:3.4,95% CI 1.3 - 9.2,P = 0.013)。在喉癌亚组中,单变量分析中TB与较差的生存期相关(HR 7.5,95% CI 1.6 - 35.6,P = 0.011),尽管在多变量模型中不显著。高TB独立预测颈部淋巴结转移(多变量OR 4.9,95% CI 1.2 - 20.5,P = 0.029),高TB患者中颈部淋巴结转移率为65.8%,低TB患者中为31.7%。高TB与晚期AJCC分期和淋巴管浸润相关。在整个队列或喉亚组中,包括TB在内,没有临床病理因素能独立预测DFS。高肿瘤芽生表示一种侵袭性HNSCC表型,可能指导选择性颈部清扫的决策。其评估简单、经济有效,对常规病理学可能有价值,有待外部验证。