He Xiaojian, Peng Xu, Duan Jianliang, Li Zongyang, Niu Yuexiang, Liu Yahui
Department of Hepatobiliary and Pancreatic Surgery, General Surgery Center, The First Hospital of Jilin University, Changchun, Jilin, China.
Discov Oncol. 2025 Aug 31;16(1):1659. doi: 10.1007/s12672-025-03406-1.
This study incorporated preoperative inflammatory scores to develop and validate a nomogram to predict overall survival in patients with hepatocellular carcinoma following curative resection.
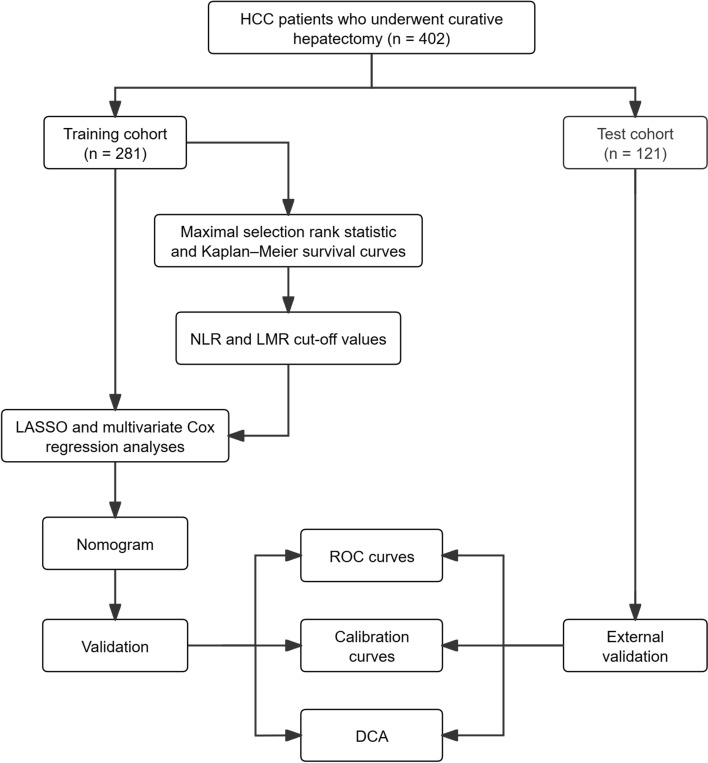
The study included 402 postoperative hepatocellular carcinoma patients, divided into training (n = 281) and test (n = 121) cohorts. Variables were analyzed using Cox proportional hazards model. The nomogram's performance was assessed using receiver operating characteristic curves, calibration curves, and decision curve analysis.
Multivariable Cox proportional hazards model analysis identified neutrophil-to-lymphocyte ratio-lymphocyte-to-monocyte ratio score (HR = 4.19, 95% CI 2.47-7.12), microvascular invasion (HR = 4.93, 95% CI 2.74-8.85), and total tumor volume (HR = 1.67, 95% CI 1.03-2.68) as independent prognostic factors (P < 0.05). The nomogram exhibited excellent discriminatory ability, with area under the curve values for 12-, 36-, and 60-month overall survival in the test cohort measuring 0.941, 0.810, and 0.881. Calibration curves verified a high degree of consistency, with a Brier score of 0.054, 0.120, and 0.102, between the predicted and observed survival probabilities in the test cohort. Decision curve analysis confirmed clinical utility across a wide threshold probability range (0.15-0.70).
The nomogram integrating neutrophil-to-lymphocyte ratio-lymphocyte-to-monocyte ratio score, microvascular invasion, and total tumor volume effectively identifies high-risk hepatocellular carcinoma patients with shorter overall survival. This tool provides clinicians with new evidence for risk-stratified interventions.
本研究纳入术前炎症评分,以开发并验证一种列线图,用于预测肝细胞癌根治性切除术后患者的总生存期。
该研究纳入402例肝细胞癌术后患者,分为训练队列(n = 281)和测试队列(n = 121)。使用Cox比例风险模型分析变量。使用受试者工作特征曲线、校准曲线和决策曲线分析评估列线图的性能。
多变量Cox比例风险模型分析确定中性粒细胞与淋巴细胞比率 - 淋巴细胞与单核细胞比率评分(HR = 4.19,95%CI 2.47 - 7.12)、微血管侵犯(HR = 4.93,95%CI 2.74 - 8.85)和肿瘤总体积(HR = 1.67,95%CI 1.03 - 2.68)为独立预后因素(P < 0.05)。列线图显示出优异的辨别能力,测试队列中12个月、36个月和60个月总生存期的曲线下面积值分别为0.941、0.810和0.881。校准曲线验证了高度一致性,测试队列中预测和观察到的生存概率之间的Brier评分为0.054、0.120和0.102。决策曲线分析证实了在广泛的阈值概率范围(0.15 - 0.70)内的临床实用性。
整合中性粒细胞与淋巴细胞比率 - 淋巴细胞与单核细胞比率评分、微血管侵犯和肿瘤总体积的列线图可有效识别总生存期较短的高危肝细胞癌患者。该工具为临床医生进行风险分层干预提供了新的证据。