Halaouate Imane, Boulahroud Imane, Eddich Yassine, Bakkali Tarik, Bounssir Ayoub, Lekehal Brahim
Vascular and Endovascular Department, CHU Ibn Sina Souissi, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco.
Int J Surg Case Rep. 2025 Oct;135:111886. doi: 10.1016/j.ijscr.2025.111886. Epub 2025 Sep 2.
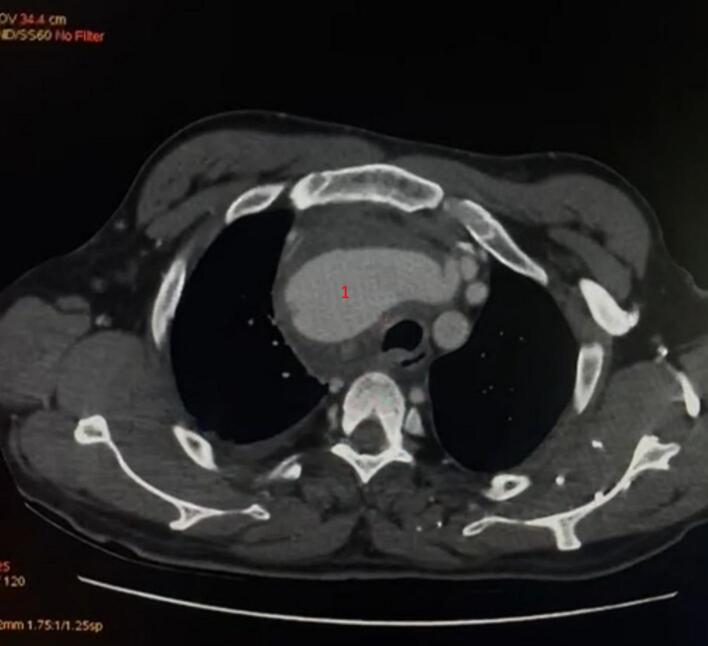
Pseudoaneurysm of the right subclavian artery is very rare, and its most serious complication is rupture, which is unpredictable and fatal. Among the infectious causes, tuberculous pseudoaneurysms represent an exceptionally rare but significant subset, arising from the direct invasion of the arterial wall by Mycobacterium tuberculosis.
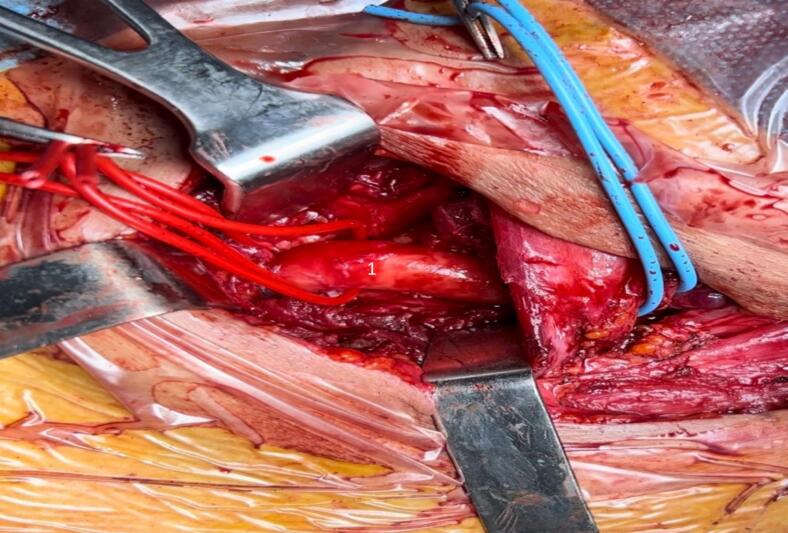
We present the case of a 60-year-old hypertensive male diagnosed with a right subclavian artery septic pseudoaneurysm, which is rare but serious, often resulting from an infection that weakens the arterial wall. Although bacterial infections are the most common etiologies, mycobacterial infections, such as those caused by Mycobacterium tuberculosis, should also be considered in regions with a high prevalence of tuberculosis or in patients with risk factors for this infection. The patient was successfully treated through a cervicotomy and challenging dissection of major neck vessels. A bypass graft between the distal right subclavian artery and the right carotid artery was performed, restoring vascular flow. Postoperative outcomes were favorable, with full recovery at one week and three months follow-up.
This case underscores the importance of timely diagnosis and surgical intervention in managing septic pseudoaneurysms, including those of tuberculous origin, to avoid life-threatening complications such as rupture or systemic sepsis. Comprehensive management should include appropriate antimicrobial therapy tailored to the underlying infectious agent to ensure long-term recovery and graft patency.
Early diagnosis is crucial to prevent the potentially life-threatening complications of a right subclavian artery pseudoaneurysm; therefore, this condition should be considered in patients with a history of trauma or infection presenting with a pulsatile supraclavicular mass or unexplained upper limb symptoms.
右锁骨下动脉假性动脉瘤非常罕见,其最严重的并发症是破裂,这种情况不可预测且会致命。在感染性病因中,结核性假性动脉瘤是一个极为罕见但重要的亚型,由结核分枝杆菌直接侵袭动脉壁引起。
我们报告一例60岁高血压男性患者,诊断为右锁骨下动脉感染性假性动脉瘤,这种情况虽罕见但严重,通常由削弱动脉壁的感染所致。尽管细菌感染是最常见的病因,但在结核病高发地区或有该感染危险因素的患者中,也应考虑结核分枝杆菌等分枝杆菌感染。该患者通过颈部切开术及对主要颈部血管进行具有挑战性的解剖得以成功治疗。在右锁骨下动脉远端与右颈动脉之间进行了搭桥移植,恢复了血管血流。术后结果良好,在一周和三个月随访时完全康复。
该病例强调了及时诊断和手术干预在处理感染性假性动脉瘤(包括结核性起源的假性动脉瘤)中的重要性,以避免诸如破裂或全身性败血症等危及生命的并发症。综合管理应包括根据潜在感染病原体进行适当的抗菌治疗,以确保长期康复和移植血管通畅。
早期诊断对于预防右锁骨下动脉假性动脉瘤潜在的危及生命的并发症至关重要;因此,对于有创伤或感染史且出现搏动性锁骨上肿块或不明原因上肢症状的患者,应考虑这种情况。