Wainwright R J
Br Heart J. 1981 Nov;46(5):465-77. doi: 10.1136/hrt.46.5.465.
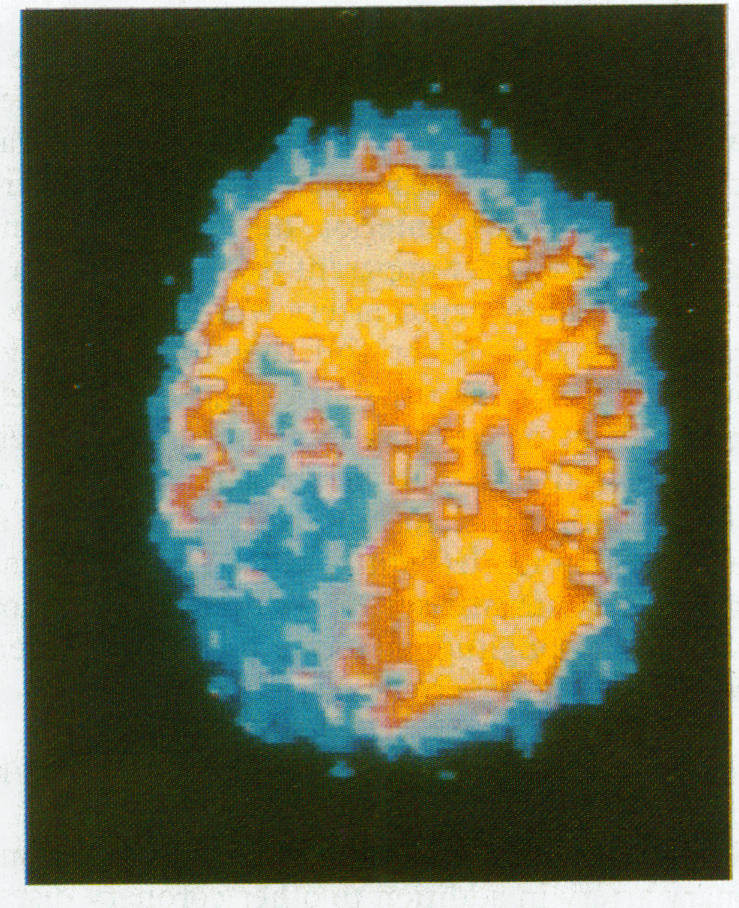
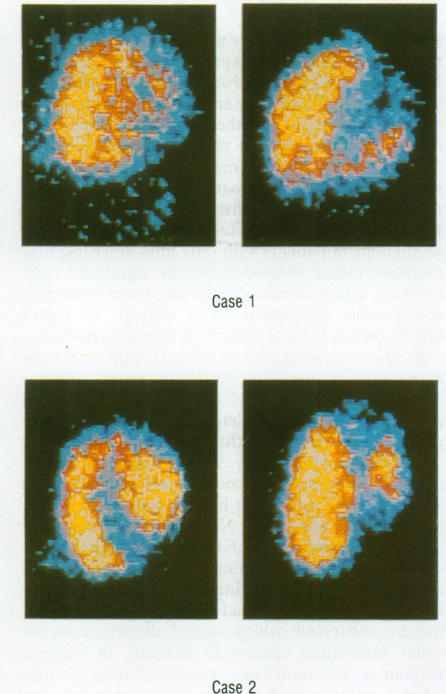
One hundred and eight patients with single and multiple vessel coronary artery disease confirmed by arteriography were evaluated by exercise thallium-201 (201Tl) myocardial scintigraphy to determine the scintigraphic appearances of specific coronary stenoses. In general proximal stenoses caused more widespread, but not necessarily more severe, myocardial tracer deficit than distal stenoses. In particular, proximal dominant right coronary artery disease was specifically associated with extensive inferior wall tracer deficit in the anterior scintigram, whereas proximal left circumflex disease caused similar tracer depletion best visualised in the left lateral scintigram. A triad of uptake defects was caused by left anterior descending coronary artery disease: viz. apical tracer deficit (anterior view) in 71% lesions, septal tracer deficit (left anterior oblique view) in 83% of lesions, and anterolateral wall tracer deficit (left lateral projection) in 72% of lesions. The last defect has been termed a 'diagonal window' because it was associated with independent disease of the main diagonal branch of the left anterior descending coronary artery or with disease in the main left anterior descending artery situated proximal to this branch. Diagonal window tracer deficit was the most useful scintigraphic sign distinguishing proximal from distal disease in the left anterior descending coronary artery. False negative scintigraphic defects occurred more commonly in patients with triple vessel disease and in association with well-developed coronary collateral vessels. Certain scintigraphic patterns of 201Tl myocardial accumulation appear invaluable in the noninvasive localisation of stenoses within specific coronary arteries and thus may be useful in predicting life-threatening coronary artery disease which should be confirmed by definite coronary arteriography. The digital 201Tl myocardial scintigram also provides an independent functional guide to the interpretation of coronary arteriograms and may be helpful in the planning of aortocoronary bypass graft surgery.
108例经动脉造影证实为单支或多支冠状动脉疾病的患者,通过运动铊-201(²⁰¹Tl)心肌闪烁显像进行评估,以确定特定冠状动脉狭窄的闪烁显像表现。一般来说,近端狭窄比远端狭窄导致更广泛但不一定更严重的心肌示踪剂缺损。特别是,近端优势型右冠状动脉疾病与前位闪烁显像中广泛的下壁示踪剂缺损特别相关,而近端左旋支疾病导致类似的示踪剂耗竭,在左侧位闪烁显像中最易观察到。左前降支冠状动脉疾病导致了一组摄取缺陷:即,71%的病变在心尖部有示踪剂缺损(前位视图),83%的病变在室间隔有示踪剂缺损(左前斜位视图),72%的病变在前外侧壁有示踪剂缺损(左侧位投影)。最后一个缺损被称为“对角窗”,因为它与左前降支冠状动脉主要对角支的独立病变或该分支近端的左前降支主干病变有关。对角窗示踪剂缺损是区分左前降支冠状动脉近端与远端疾病最有用的闪烁显像征象。假阴性闪烁显像缺损在三支血管疾病患者中更常见,并且与发达的冠状动脉侧支血管有关。²⁰¹Tl心肌摄取的某些闪烁显像模式在特定冠状动脉狭窄的无创定位中似乎非常有价值,因此可能有助于预测应通过明确的冠状动脉造影确诊的危及生命的冠状动脉疾病。数字化²⁰¹Tl心肌闪烁显像还为冠状动脉造影的解读提供了独立的功能指导,并且可能有助于主动脉冠状动脉搭桥手术的规划。