Wanebo H J, Koness R J, Vezeridis M P, Cohen S I, Wrobleski D E
Department of Surgery, Brown University, Providence, Rhode Island.
Ann Surg. 1994 Oct;220(4):586-95; discussion 595-7. doi: 10.1097/00000658-199410000-00017.
The authors describe their experience with pelvic resection of recurrent rectal cancer with emphasis on patient selection for curative intent based on known tumor risk factors.
Pelvic recurrence is a formidable problem in 30% of patients who have undergone a curative resection of primary rectal cancer. Although radiation can reduce the development of local recurrence and can provide palliation to many patients with localized disease, it is not curative. The authors and others have used the technique of abdominal sacral resection (ABSR) with or without pelvic exenteration to resect pelvic recurrence and its musculoskeletal extensions in selected patients with satisfactory long-term survival.
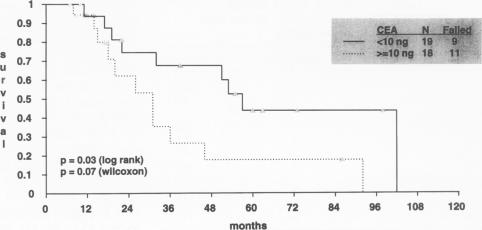
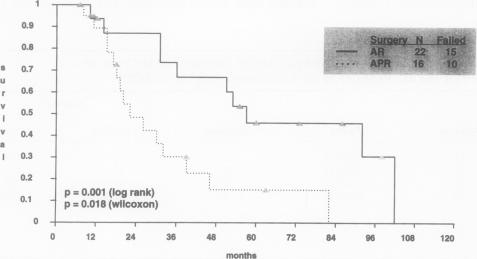
The technique of ABSR with or without pelvic exenteration or resection of pelvic viscera, which the authors have described previously, was used in 53 patients with recurrent rectal cancer--47 patients for curative intent and 6 for palliation. Previous surgeries were abdominal perineal resections (APRs) in 26 patients, anterior resections in 19 patients, and other procedures in 2 patients; original primary Dukes' stage was B in 52% and C in 48%. Almost all patients had been irradiated previously, generally in the 4000 to 5900 cGy range. Preoperative carcinoembryonic antigen (CEA) levels (before ABSR) were elevated (> 5 ng/mL) in 54%.
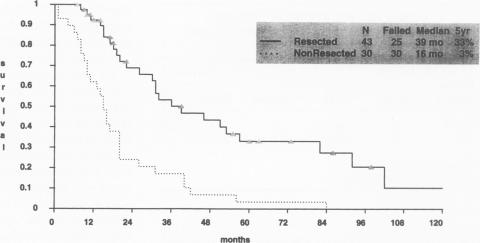
Postoperative morbidity was encountered in most patients. Mortality was 8.5% in the curative group. Long-term survival for 4 years was achieved in 14 of 43 patients (33%), and 10 patients were alive with an acceptable quality of life after 5 years. Patients who had previous anterior resections or whose preoperative CEA levels were less than 10 ng/mL had a survival rate of approximately 45%, whereas patients with previous APRs and preoperative CEA levels greater than 10 ng/mL had a survival rate of only 15% to 18%. Patients with bone marrow invasion, positive margins, or pelvic node metastases had a median survival of only 10 months.
Pelvic recurrence of rectal cancer can be resected safely with expectation of long-term survival of 33%. Patient selection based on known risk factors can identify patients most likely to benefit from resection and eliminate those who should be treated for palliation only.
作者描述了他们对复发性直肠癌进行盆腔切除术的经验,重点是基于已知肿瘤风险因素选择有治愈意图的患者。
盆腔复发是30%接受原发性直肠癌根治性切除患者面临的一个棘手问题。尽管放疗可以减少局部复发的发生,并能为许多局限性疾病患者提供姑息治疗,但它并不能治愈。作者和其他人已采用腹骶切除术(ABSR)技术,无论是否行盆腔脏器清除术,对部分患者切除盆腔复发灶及其肌肉骨骼侵犯部分,取得了满意的长期生存效果。
作者之前描述的ABSR技术,无论是否行盆腔脏器清除术或盆腔脏器切除术,应用于53例复发性直肠癌患者,其中47例有治愈意图,6例为姑息治疗。既往手术包括26例腹会阴联合切除术(APR)、19例前切除术和2例其他手术;原发病灶Dukes分期B期占52%,C期占48%。几乎所有患者此前均接受过放疗,剂量一般在4000至5900 cGy范围内。术前癌胚抗原(CEA)水平(ABSR术前)升高(>5 ng/mL)的患者占54%。
大多数患者术后出现并发症。治愈组死亡率为8.5%。43例患者中有14例(33%)实现了4年长期生存,10例患者在5年后存活,生活质量尚可。既往接受前切除术或术前CEA水平低于10 ng/mL的患者生存率约为45%,而既往接受APR且术前CEA水平高于10 ng/mL的患者生存率仅为15%至18%。有骨髓侵犯、切缘阳性或盆腔淋巴结转移的患者中位生存期仅为10个月。
直肠癌盆腔复发可以安全切除,预期长期生存率为33%。基于已知风险因素进行患者选择,可以识别出最有可能从切除术中获益的患者,并排除那些仅应接受姑息治疗的患者。