Veress B, Löfberg R, Bergman L
Department of Pathology, Karolinska Institute, Huddinge University Hospital, Sweden.
Gut. 1995 Jun;36(6):880-6. doi: 10.1136/gut.36.6.880.
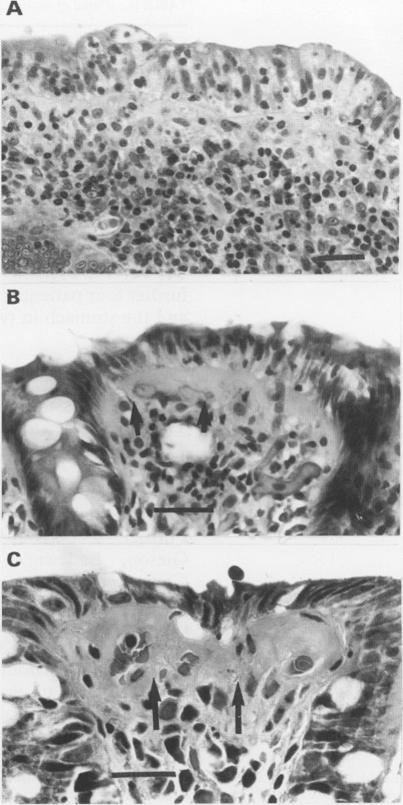
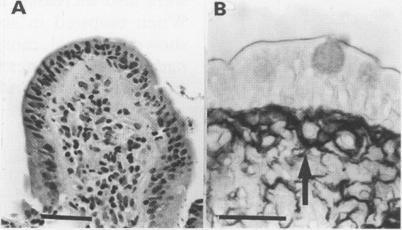
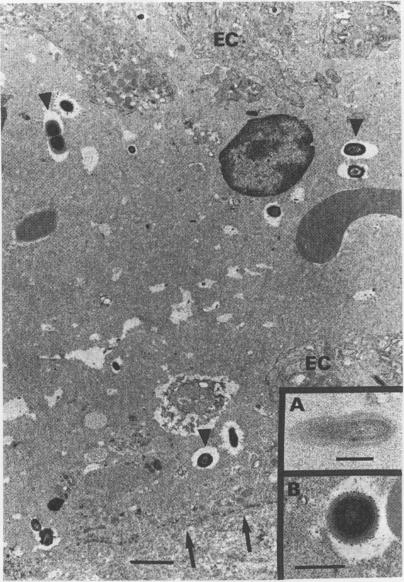
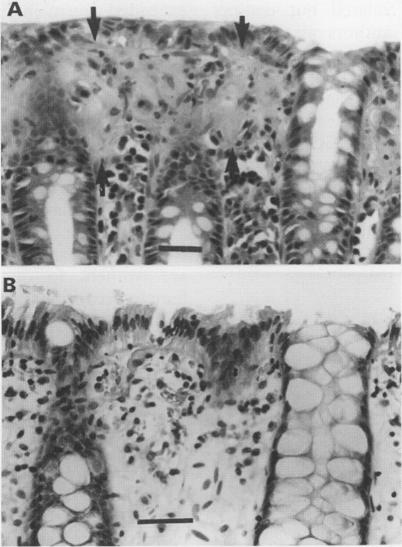
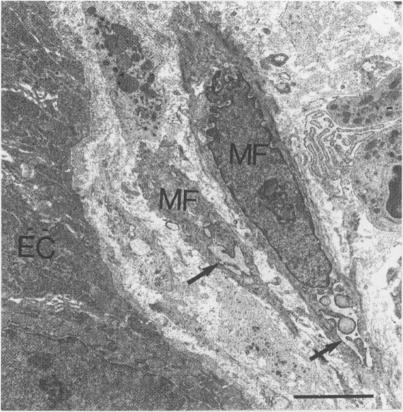
The colorectal biopsy specimens from 30 patients with chronic watery diarrhoea but normal endoscopic and radiographic findings were studied by light microscopy, morphometry, immunohistochemistry, and two patients with electron microscopy. The histological changes in the colorectum were originally diagnosed in six patients as lymphocytic colitis and in 24 patients as collagenous colitis. The analysis of the specimens for this study could delineate three distinct groups of microscopic colitis: lymphocytic colitis (six patients), collagenous colitis without lymphocytic attack on the surface epithelium (seven patients), and a mixed form presenting with both thickening of the collagen plate and increased number of intraepithelial lymphocytes (17 patients). No transformation was seen from one type to another during follow up of six patients for four to seven years. Increased numbers of active pericryptal myofibroblasts were found with the electron microscope in one patient with mixed microscopic colitis showing also myofibroblasts entrapped within the collagen layer. Hitherto undescribed flat mucosa of the ileum was found in one patient with lymphocytic colitis and both flat mucosa and thickening of the collagen plate in the ileum were seen in one patient with the mixed form of the disease. In another patient with mixed microscopic colitis, normalisation of the colorectal morphology occurred after temporary loop ileostomy, followed by the reappearance of both diarrhoea, inflammation, and thickening of the collagen plate after the ileostomy was reversed. No association was found between non-steroid anti-inflammatory drug (NSAID) consumption and collagenous or mixed microscopic colitis. The primary cause of microscopic colitis is probably an immunological reaction to luminal antigen/s, perhaps of ileal origin. The engagement of the pericryptal myofibroblasts in the disease process might result in the development of the various forms of microscopic colitis. An inverse relation between intraepithelial lymphocyte count and collagen thickness may indicate that microscopic colitis is a spectral disease.
对30例慢性水样腹泻但内镜及影像学检查结果正常的患者的结肠活检标本进行了光镜、形态计量学、免疫组织化学研究,对其中2例患者进行了电镜检查。结肠的组织学改变最初在6例患者中诊断为淋巴细胞性结肠炎,在24例患者中诊断为胶原性结肠炎。本研究标本分析可区分出三种不同类型的显微镜下结肠炎:淋巴细胞性结肠炎(6例)、无表面上皮淋巴细胞浸润的胶原性结肠炎(7例)以及同时出现胶原板增厚和上皮内淋巴细胞增多的混合形式(17例)。6例患者随访4至7年期间未见一种类型转变为另一种类型。在1例混合性显微镜下结肠炎患者中,电镜发现活跃的隐窝周围肌成纤维细胞数量增加,且肌成纤维细胞被困于胶原层内。在1例淋巴细胞性结肠炎患者中发现了此前未描述过的回肠扁平黏膜,在1例混合性疾病患者中可见回肠扁平黏膜及胶原板增厚。在另1例混合性显微镜下结肠炎患者中,临时回肠造口术后结肠形态恢复正常,但回肠造口还纳后腹泻、炎症及胶原板增厚又再次出现。未发现非甾体抗炎药(NSAID)使用与胶原性或混合性显微镜下结肠炎之间存在关联。显微镜下结肠炎的主要病因可能是对腔内抗原(可能源自回肠)的免疫反应。隐窝周围肌成纤维细胞参与疾病过程可能导致各种形式的显微镜下结肠炎的发生。上皮内淋巴细胞计数与胶原厚度之间的负相关可能表明显微镜下结肠炎是一种谱系疾病。