Van Laethem J L, Vertongen P, Deviere J, Van Rampelbergh J, Rickaert F, Cremer M, Robberecht P
Department of Hepatogastroenterology, Université Libre de Bruxelles, Belgium.
Gut. 1995 May;36(5):781-7. doi: 10.1136/gut.36.5.781.
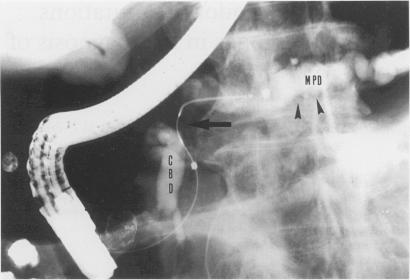
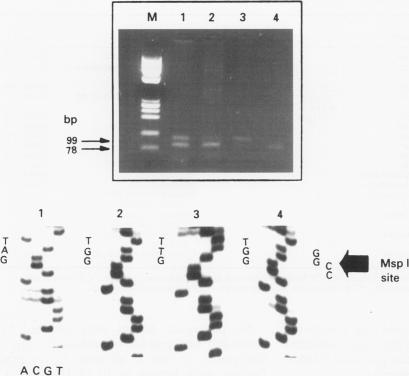
Differential diagnosis of pancreatic cancer and chronic pancreatitis is sometimes difficult and cytological examination of brushings or aspirated material collected during endoscopic retrograde cholangiopancreatography (ERCP) remains disappointing. As point mutations in codon 12 of the c-Ki-ras 2 gene are found in most pancreatic adenocarcinoma and not in chronic pancreatitis, this study analysed prospectively the presence of these mutations in brushing samples collected during ERCP in 45 patients (26 males, 19 females) showing a dominant stricture of the main pancreatic duct at pancreatography: 24 with pancreatic adenocarcinoma, 16 with chronic pancreatitis, and five intraductal mucin hypersecreting neoplasms. Twenty of 45 patients presented equivocal ERCP findings that did not permit a definite diagnosis. Ki-ras mutations at codon 12 were detected using a rapid and sensitive method based on polymerase chain reaction mediated restriction fragment length polymorphism analysis and confirmed by direct sequencing of polymerase chain reaction products. Results were compared with those provided by routine brush cytology. A definitive diagnosis was established for each patient. Mutations were detected in 20 of 24 patients with pancreatic adenocarcinoma (83%), but in none of the chronic pancreatitis patients and intraductal mucin hypersecreting neoplasms, irrespective of their location. By contrast, only 13 of 24 pancreatic adenocarcinoma (54%) were detected by conventional cytological examination, which yielded four false negative and seven non-contributive results. Sensitivity, specificity, and accuracy of molecular biological and cytological methods were 83%-76%, 100-83%, and 90%-58%, respectively. Notably the mutations could be detected in six patients with small tumour size (< or = 2 cm). In conclusion, Ki-ras analysis performed on pancreatic brushing samples is an efficient procedure, more accurate than cytology in the diagnosis of pancreatic adenocarcinoma, and highly specific in the differentiation between neoplastic and chronic inflammatory ductal changes, especially in patients showing inconclusive ERCP findings.
胰腺癌与慢性胰腺炎的鉴别诊断有时存在困难,在内镜逆行胰胆管造影(ERCP)期间收集的刷检物或吸出物的细胞学检查结果仍不尽人意。由于在大多数胰腺腺癌中可发现c-Ki-ras 2基因第12密码子的点突变,而慢性胰腺炎中未发现,本研究前瞻性分析了45例(26例男性,19例女性)在胰胆管造影时表现为主胰管显性狭窄患者的ERCP期间收集的刷检样本中这些突变的存在情况:24例为胰腺腺癌,16例为慢性胰腺炎,5例为导管内黏液高分泌性肿瘤。45例患者中有20例ERCP检查结果不明确,无法做出明确诊断。使用基于聚合酶链反应介导的限制性片段长度多态性分析的快速灵敏方法检测第12密码子的Ki-ras突变,并通过聚合酶链反应产物的直接测序进行确认。将结果与常规刷检细胞学检查结果进行比较。为每位患者确立了明确诊断。在24例胰腺腺癌患者中有20例(83%)检测到突变,但慢性胰腺炎患者和导管内黏液高分泌性肿瘤患者均未检测到突变,无论其位置如何。相比之下,常规细胞学检查仅检测出24例胰腺腺癌中的13例(54%),产生了4例假阴性和7例无诊断价值的结果。分子生物学方法和细胞学方法的敏感性、特异性和准确性分别为83% - 76%、100% - 83%和90% - 58%。值得注意的是,在6例肿瘤较小(≤2 cm)的患者中也检测到了突变。总之,对胰腺刷检样本进行Ki-ras分析是一种有效的方法,在胰腺腺癌诊断中比细胞学更准确,在肿瘤性和慢性炎症性导管改变的鉴别中具有高度特异性,尤其是在ERCP检查结果不明确的患者中。