Zimmer T, Ziegler K, Bäder M, Fett U, Hamm B, Riecken E O, Wiedenmann B
Department of Internal Medicine, Steglitz Medical Centre, Free University of Berlin, Germany.
Gut. 1994 Apr;35(4):471-5. doi: 10.1136/gut.35.4.471.
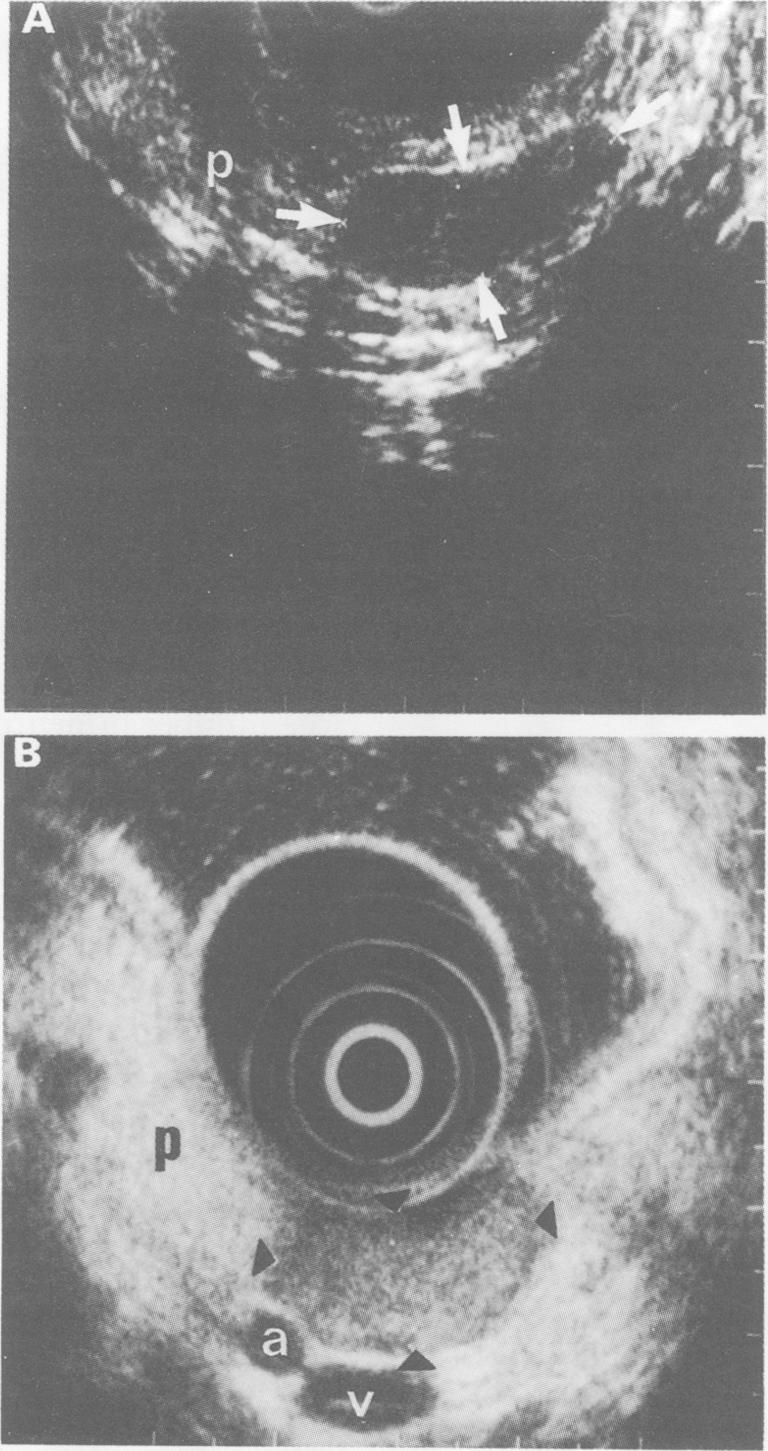
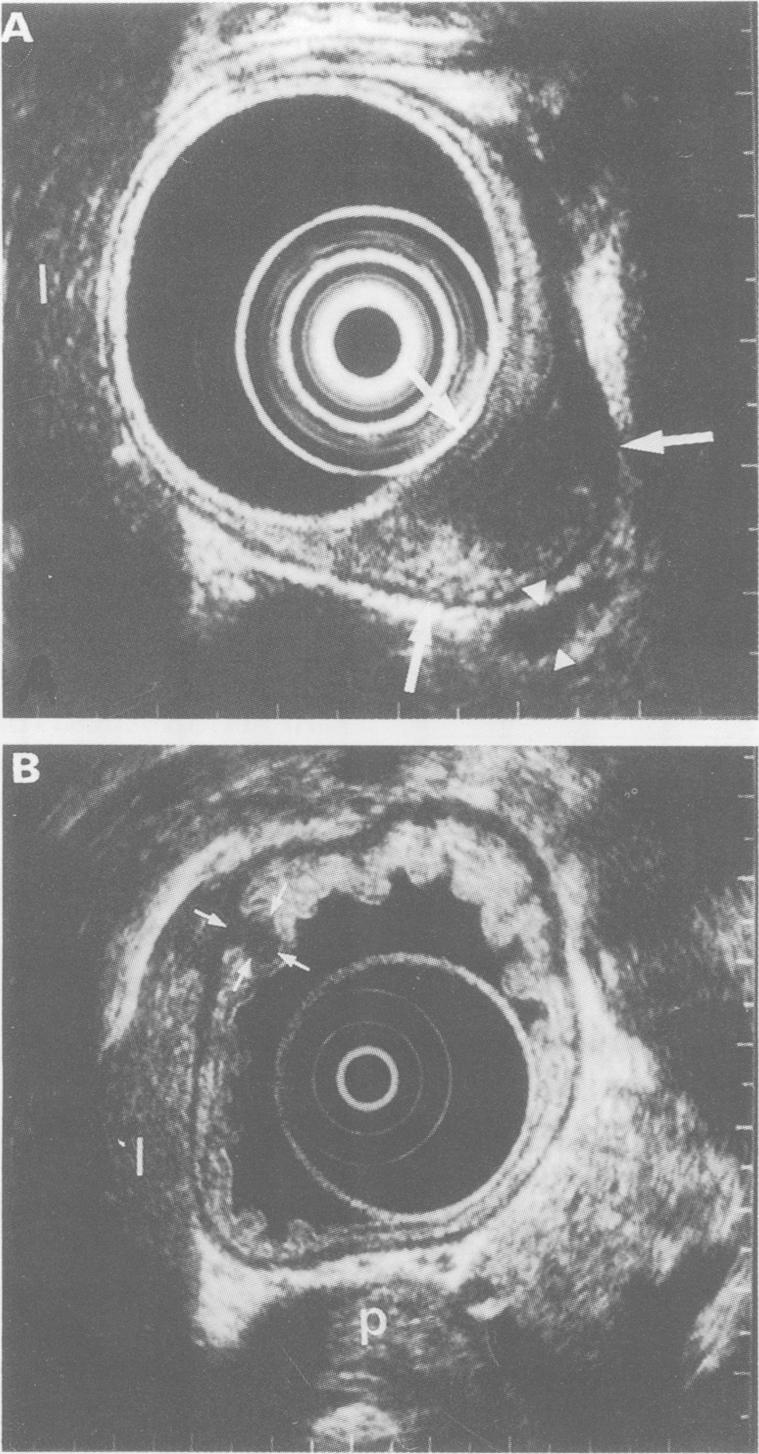
In order to localise neuroendocrine tumours of the foregut type (that is, of the stomach, duodenum, and pancreas), 18 patients were studied prospectively by endoscopic ultrasonography, computed tomography, transabdominal ultrasonography, magnetic resonance imaging, and somatostatin receptor scintigraphy. These 18 patients had a total of 25 primary tumour lesions which were verified histologically in tissue obtained by surgery or by ultrasound or endoscopy guided biopsy. Tumours were found in the stomach (n = 1), duodenum (n = 6), pancreas (n = 17), and liver (n = 1). Endoscopic ultrasonography had the highest sensitivity for tumour detection, followed by somatostatin receptor scintigraphy, computed tomography, transabdominal ultrasonography, and magnetic resonance imaging (88%, 52%, 36%, 32%, and 24% respectively). Endoscopic ultrasonography was especially sensitive in tumours smaller than 2 cm in diameter (88% v somatostatin receptor scintigraphy 35%; computed tomography 12%; transabdominal ultrasonography 6%; and magnetic resonance imaging 0%). Of 17 tumours located in the pancreas, endoscopic ultrasonography showed a sensitivity of 94% (somatostatin receptor scintigraphy 47%; computed tomography 47%; transabdominal ultrasonography 41%; and magnetic resonance imaging 29%). Of eight extrapancreatic tumours, six were identified by endoscopic ultrasonography, five by somatostatin receptor scintigraphy, and only one by computed tomography, transabdominal ultrasonography, and magnetic resonance imaging. One neuroendocrine tumour that was not detected by endoscopic ultrasonography was correctly identified by somatostatin receptor scintigraphy. Endoscopic ultrasound allowed correct determination of the tumour size and tumour spread into parapancreatic structures, especially the large vessels (T stage), in all 14 patients operated upon. The lymph node stage (N stage) was correctly determined in 10 of these 14 patients. In summary, endoscopic ultrasonography and somatostatin receptor scintigraphy were the most sensitive imaging methods for the localisation of these tumours and should be used as early diagnostic procedures to accurately stage neuroendocrine tumours of the foregut type.
为了定位前肠型神经内分泌肿瘤(即胃、十二指肠和胰腺的神经内分泌肿瘤),我们对18例患者进行了前瞻性研究,采用了内镜超声检查、计算机断层扫描、经腹超声检查、磁共振成像和生长抑素受体闪烁显像。这18例患者共有25个原发性肿瘤病灶,这些病灶通过手术获取的组织或超声或内镜引导下活检获得的组织进行了组织学验证。肿瘤分别位于胃(n = 1)、十二指肠(n = 6)、胰腺(n = 17)和肝脏(n = 1)。内镜超声检查对肿瘤检测的敏感性最高,其次是生长抑素受体闪烁显像、计算机断层扫描、经腹超声检查和磁共振成像(分别为88%、52%、36%、32%和24%)。内镜超声检查对直径小于2 cm的肿瘤尤其敏感(88%,而生长抑素受体闪烁显像为35%;计算机断层扫描为12%;经腹超声检查为6%;磁共振成像为0%)。在位于胰腺的17个肿瘤中,内镜超声检查的敏感性为94%(生长抑素受体闪烁显像为47%;计算机断层扫描为47%;经腹超声检查为41%;磁共振成像为29%)。在8个胰腺外肿瘤中,6个通过内镜超声检查得以识别,5个通过生长抑素受体闪烁显像得以识别,而通过计算机断层扫描、经腹超声检查和磁共振成像仅识别出1个。1个未被内镜超声检查检测到的神经内分泌肿瘤通过生长抑素受体闪烁显像得以正确识别。在所有接受手术的14例患者中,内镜超声检查能够正确确定肿瘤大小以及肿瘤向胰腺旁结构尤其是大血管的扩散情况(T分期)。在这14例患者中有10例正确确定了淋巴结分期(N分期)。总之,内镜超声检查和生长抑素受体闪烁显像对于这些肿瘤的定位是最敏感的成像方法,应作为早期诊断程序用于准确分期前肠型神经内分泌肿瘤。