Rao N A, Hidayat A
Doheny Eye Institute, Los Angeles, USA.
Trans Am Ophthalmol Soc. 2000;98:183-93; discussion 193-4.
Endophthalmitis caused by endogenous Candida and Aspergillus species has emerged as a visually threatening complication in patients with immune deficiency of various causes. Twenty-five patients who underwent enucleation, 13 with endogenous Aspergillus endophthalmitis and 12 with endogenous Candida intraocular infections, were evaluated. Both clinical features and intraocular spread of the fungi were studied to determine which clinical and/or histopathologic features could help distinguish aspergillosis from Candida infections.
Clinical information was sought from each case to determine whether there was any underlying systemic condition and to delineate the characteristic clinical features seen at initial presentation. The results of vitreous and other tissue cultures for bacteria and fungi were evaluated. Patients with AIDS were excluded. The enucleated globes were processed for histopathologic analysis to detect location of the fungal elements, inflammatory response, and vascular invasion by the fungi.
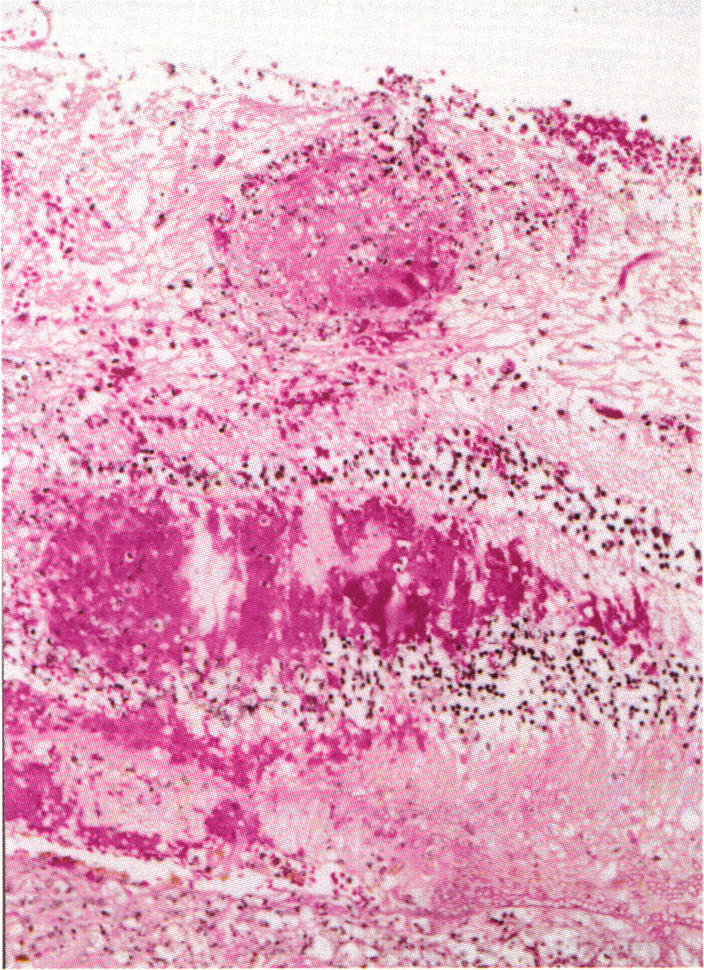
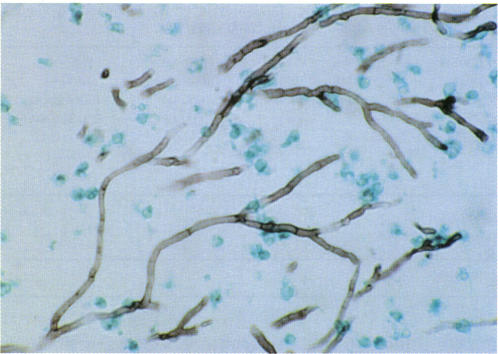
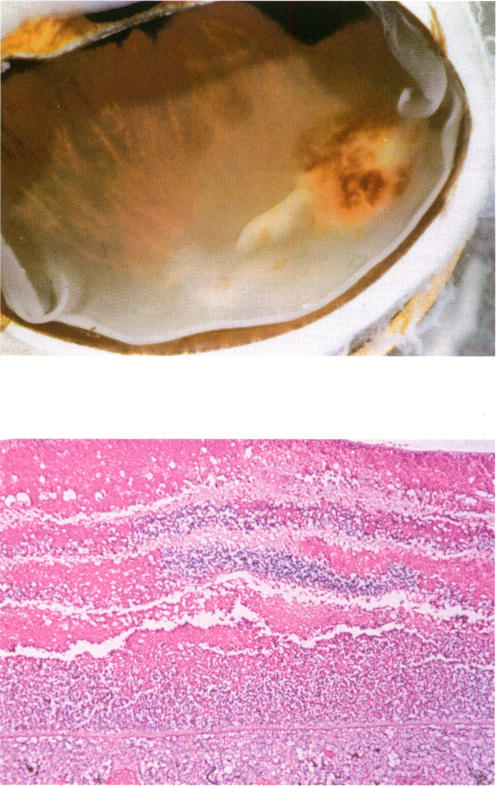
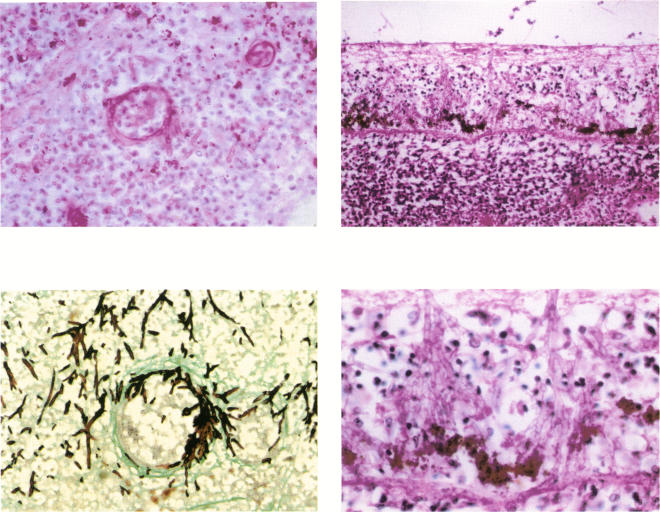
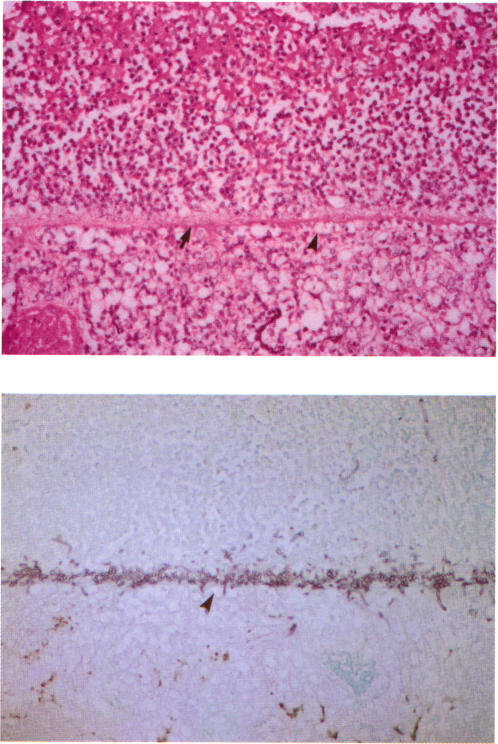
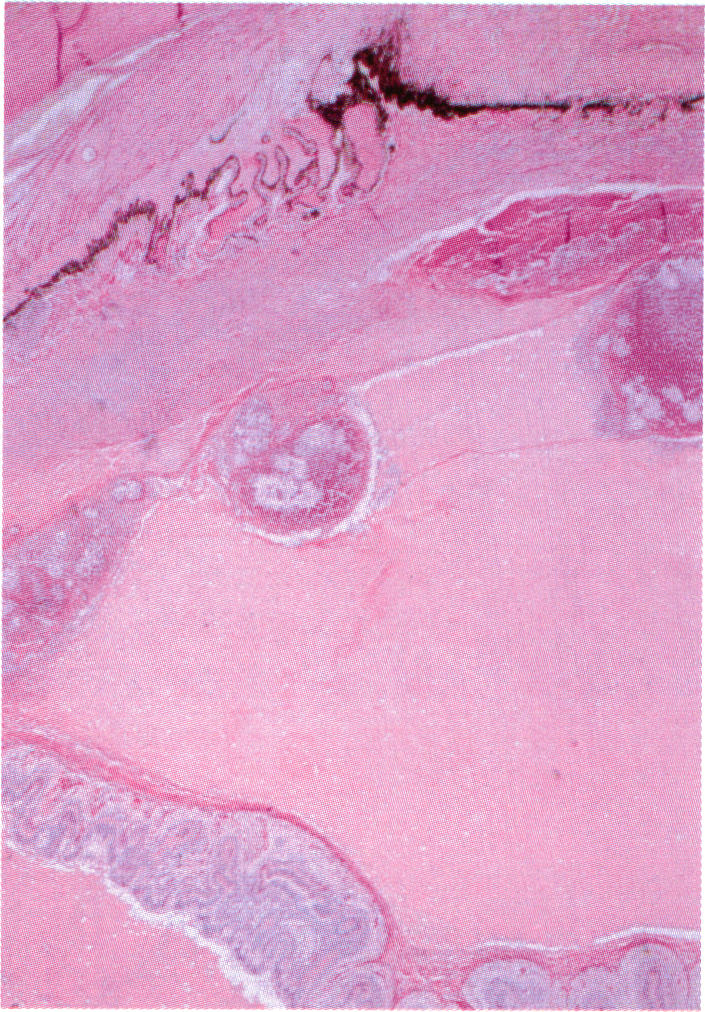
With respect to the various predisposing systemic conditions, Candida species endophthalmitis was noted in patients with a history of gastrointestinal surgery, hyperalimentation, or diabetes mellitus, whereas aspergillosis was present in patients who had undergone organ transplantation or cardiac surgery. The vitreous was the primary focus of infection for Candida, whereas subretinal or sub-retinal pigment epithelium infection was noted in eyes with aspergillosis. Retinal and choroidal vessel wall invasion by fungal elements was noted in cases of aspergillosis but not in cases with candidiasis. The high rate of cerebral and cardiac infection in patients with Aspergillus endophthalmitis was not seen in those with Candida infection.
The present study indicates that unlike Candida endophthalmitis, aspergillosis is seen in organ transplant or cardiac surgery patients, and its initial clinical presentation includes extensive areas of deep retinitis/choroiditis. Contrary to the findings in Candida endophthalmitis, vitreous biopsy may not yield positive results in aspergillosis. Aspergillus endophthalmitis is usually associated with a high rate of mortality caused by cerebral and cardiac complications.
由内源性念珠菌和曲霉菌引起的眼内炎已成为各种原因导致免疫缺陷患者视力威胁性并发症。对25例行眼球摘除术的患者进行了评估,其中13例患有内源性曲霉菌性眼内炎,12例患有内源性念珠菌性眼内感染。研究了真菌的临床特征和眼内播散情况,以确定哪些临床和/或组织病理学特征有助于区分曲霉菌病和念珠菌感染。
从每个病例中获取临床信息,以确定是否存在任何潜在的全身状况,并描述初次就诊时所见的特征性临床特征。评估玻璃体和其他组织的细菌和真菌培养结果。排除艾滋病患者。对摘除的眼球进行组织病理学分析,以检测真菌成分的位置、炎症反应和真菌的血管侵袭情况。
关于各种易感全身状况,念珠菌性眼内炎见于有胃肠道手术、胃肠外营养或糖尿病病史的患者,而曲霉菌病见于接受器官移植或心脏手术的患者。玻璃体是念珠菌感染的主要部位,而曲霉菌性眼内炎患者的视网膜下或视网膜色素上皮下感染较为常见。曲霉菌病患者可见真菌成分侵袭视网膜和脉络膜血管壁,而念珠菌病患者未见此情况。曲霉菌性眼内炎患者的脑和心脏感染率较高,念珠菌感染患者则未出现这种情况。
本研究表明,与念珠菌性眼内炎不同,曲霉菌病见于器官移植或心脏手术患者,其初始临床表现包括广泛的深层视网膜炎/脉络膜炎区域。与念珠菌性眼内炎的结果相反,玻璃体活检在曲霉菌病中可能不会得出阳性结果。曲霉菌性眼内炎通常与脑和心脏并发症导致的高死亡率相关。