Kreimeier U
Ludwig-Maximilians-Universität München, Munich, Germany.
Crit Care. 2000;4 Suppl 2(Suppl 2):S3-7. doi: 10.1186/cc968. Epub 2000 Oct 13.
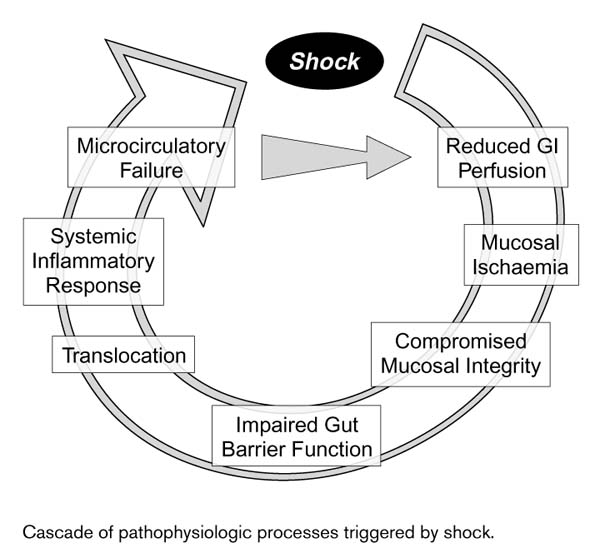
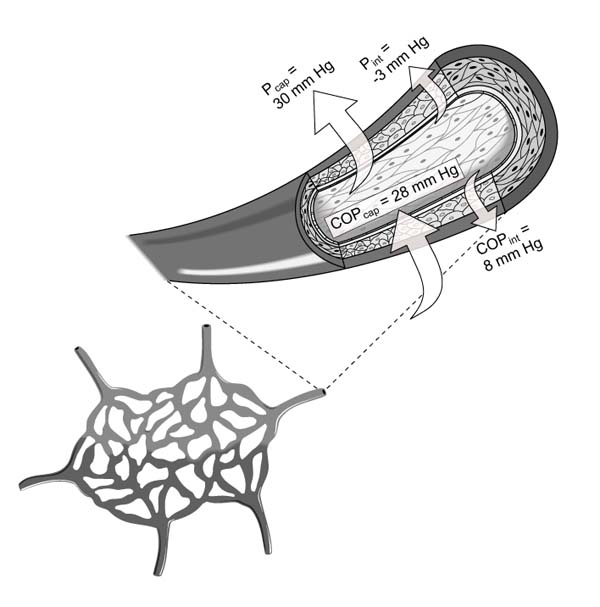
Fluid imbalance can arise due to hypovolemia, normovolemia with maldistribution of fluid, and hypervolemia. Trauma is among the most frequent causes of hypovolemia, with its often profuse attendant blood loss. Another common cause is dehydration, which primarily entails loss of plasma rather than whole blood. The consequences of hypovolemia include reduction in circulating blood volume, lower venous return and, in profound cases, arterial hypotension. Myocardial failure may result from increased myocardial oxygen demand in conjunction with reduced tissue perfusion. Finally, anaerobic metabolism due to reduced perfusion may produce acidosis and, together with myocardial dysfunction, precipitate multi-organ failure. The splanchnic organs are particularly susceptible to the deleterious effects of hypotension and hypovolemic shock, and these effects, depending upon their duration and severity, may be irreversible despite restoration of normovolemia by fluid administration. Patient monitoring in the intensive care unit typically relies upon central venous pressure devices, whereas the primary focus in the operating theater is blood volume deficit estimated from suction devices. However, estimates of intraoperative blood loss can be inaccurate, potentially leading to inappropriate fluid management. Normovolemia with maldistribution of fluid can be encountered in shock-specific microcirculatory disorders secondary to hypovolemia, as well as pain and stress. Consequent vasoconstriction and reduced tissue driving pressure, as well as leukocyte and platelet adhesion, and liberation of humoral and cellular mediators, may impair or abolish blood flow in certain areas. The localized perfusion deficit may contribute to multi-organ failure. Choice of resuscitation fluid may be important in this context, since some evidence suggests that at least certain colloids might be helpful in diminishing post-ischemic microvascular leukocyte adherence. Excessive volume administration may lead to fluid overload and associated impairment of pulmonary function. However, entry of fluid into the lungs may also be facilitated by increased vascular permeability in certain pathologic conditions, especially sepsis and endotoxemia, even in the absence of substantially rising hydrostatic pressure. Another condition associated with elevated vascular permeability is systemic capillary leak syndrome. The chief goal of fluid management, based upon current understanding of the pathophysiology of fluid imbalance, should be to ensure adequate oxygen delivery by optimizing blood oxygenation, perfusion pressure, and circulating volume.
液体失衡可由低血容量、液体分布异常的正常血容量以及高血容量引起。创伤是低血容量最常见的原因之一,常伴有大量失血。另一个常见原因是脱水,主要导致血浆而非全血丢失。低血容量的后果包括循环血量减少、静脉回流降低,严重时会出现动脉低血压。心肌需氧量增加并伴有组织灌注减少可能导致心肌衰竭。最后,灌注减少引起的无氧代谢可能产生酸中毒,并与心肌功能障碍一起,引发多器官功能衰竭。内脏器官对低血压和低血容量性休克的有害影响尤为敏感,这些影响,取决于其持续时间和严重程度,即使通过补液恢复了正常血容量,也可能是不可逆的。重症监护病房对患者的监测通常依赖中心静脉压装置,而手术室的主要关注点是根据吸引装置估计的血容量不足。然而,术中失血量的估计可能不准确,可能导致液体管理不当。液体分布异常的正常血容量可出现在低血容量继发的特定休克微循环障碍以及疼痛和应激中。随之而来的血管收缩、组织驱动压力降低,以及白细胞和血小板黏附,还有体液和细胞介质的释放,可能会损害或消除某些区域的血流。局部灌注不足可能导致多器官功能衰竭。在这种情况下,复苏液体的选择可能很重要,因为一些证据表明,至少某些胶体可能有助于减少缺血后微血管白细胞黏附。过量补液可能导致液体过载和相关的肺功能损害。然而,在某些病理状态下,尤其是脓毒症和内毒素血症,即使没有明显升高的静水压,血管通透性增加也可能促使液体进入肺部。另一种与血管通透性升高相关的情况是系统性毛细血管渗漏综合征。基于目前对液体失衡病理生理学的理解,液体管理的主要目标应该是通过优化血液氧合、灌注压力和循环血量来确保充足的氧输送。