Beales I L
Medical School, University of East Anglia, Norwich NR74 7TJ, United Kindgom.
BMC Gastroenterol. 2001;1:7. doi: 10.1186/1471-230x-1-7. Epub 2001 Aug 10.
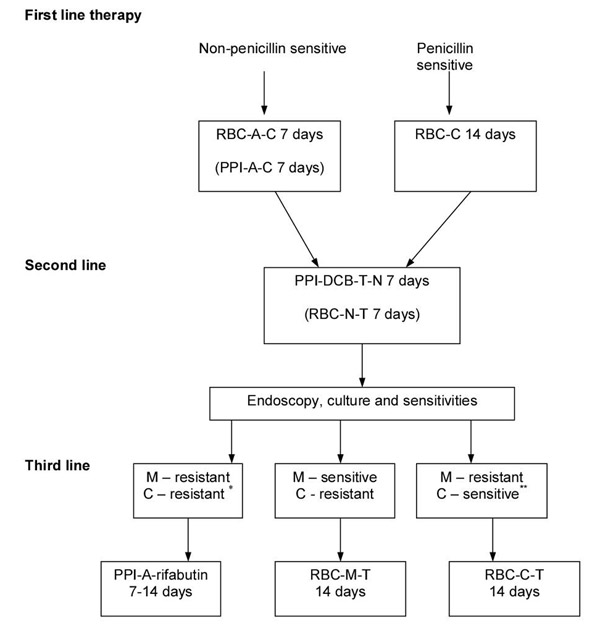
Many Helicobacter pylori eradication regimens have been described. There are little data reporting their efficacy or integration in routine clinical practice. The overall results of eradication therapy in a cohort of patients are described and an algorithm for management outlined.
469 patients receiving eradication therapy in routine clinical practice were evaluated. The successes of individual regimes as first, second and third line therapy were determined.
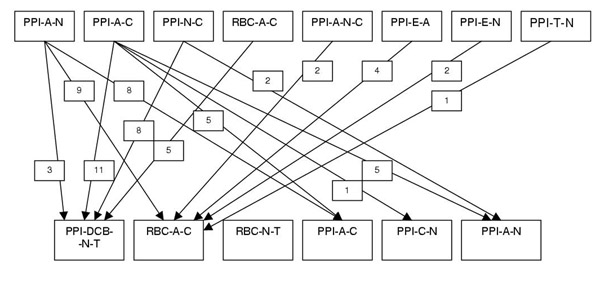
Overall success after one, two and three courses of therapy were 73% (95% confidence intervals 69-77%), 94% (91-96%) and 98% (97-99%) respectively. 10 different regimens, including many non-recommended ones were used as primary therapy. Ranitidine bismuth citrate-amoxicillin-clarithromycin triple therapy (94.8%, 90-99%) was significantly more effective than any other combination as primary therapy, including all proton pump inhibitor based triple therapies. Quadruple therapy with bismuth chelate-proton pump inhibitor-tetracycline and a nitroimidazole (70%, 52-88%) and ranitidine bismuth citrate-based triple therapy (73%, 56-90%) where more effective second line combinations than proton pump inhibitor-triple therapies (37.5%, 12-58%). Third line therapy directed by the results of sensitivity testing improved eradication compared to further empirical antibiotics. The use of a proton pump inhibitor with clarithromycin and a nitroimidazole as initial therapy was associated with a significantly worse overall eradication rate than other combinations.
Helicobacter pylori eradication rates can be maximised by using ranitidine bismuth citrate-clarithromycin-amoxicillin containing triple therapy, followed by bismuth and nitroimidazle containing second-line therapy, with third line combinations directed by sensitivity testing. Proton pump inhibitor-clarithromycin-metronidazole combinations should be avoided.
已描述了多种幽门螺杆菌根除方案。但关于这些方案在常规临床实践中的疗效或整合应用的数据较少。本文描述了一组患者根除治疗的总体结果,并概述了一种管理算法。
对469例在常规临床实践中接受根除治疗的患者进行评估。确定了作为一线、二线和三线治疗的各个方案的成功率。
一疗程、二疗程和三疗程治疗后的总体成功率分别为73%(95%置信区间69 - 77%)、94%(91 - 96%)和98%(97 - 99%)。10种不同的方案,包括许多未被推荐的方案,被用作初始治疗。枸橼酸铋雷尼替丁 - 阿莫西林 - 克拉霉素三联疗法(94.8%,90 - 99%)作为初始治疗比任何其他组合,包括所有基于质子泵抑制剂的三联疗法,显著更有效。铋螯合物 - 质子泵抑制剂 - 四环素和硝基咪唑的四联疗法(70%,52 - 88%)以及枸橼酸铋雷尼替丁为基础的三联疗法(73%,56 - 90%)作为二线组合比质子泵抑制剂 - 三联疗法(37.5%,12 - 58%)更有效。与进一步的经验性抗生素治疗相比,根据药敏试验结果指导的三线治疗提高了根除率。使用质子泵抑制剂联合克拉霉素和硝基咪唑作为初始治疗与总体根除率显著低于其他组合相关。
通过使用含枸橼酸铋雷尼替丁 - 克拉霉素 - 阿莫西林的三联疗法,随后使用含铋和硝基咪唑的二线疗法,并根据药敏试验指导三线组合,可使幽门螺杆菌根除率最大化。应避免使用质子泵抑制剂 - 克拉霉素 - 甲硝唑组合。