Silman Alan J, Pearson Jacqueline E
ARC Epidemiology Unit, School of Epidemiology & Health Sciences, University of Manchester, UK.
Arthritis Res. 2002;4 Suppl 3(Suppl 3):S265-72. doi: 10.1186/ar578. Epub 2002 May 9.
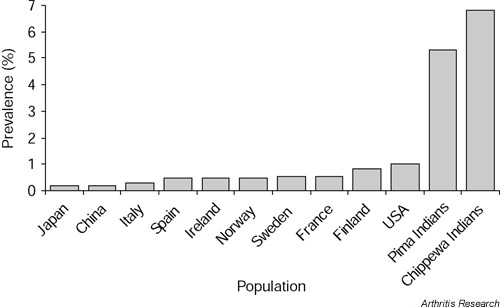
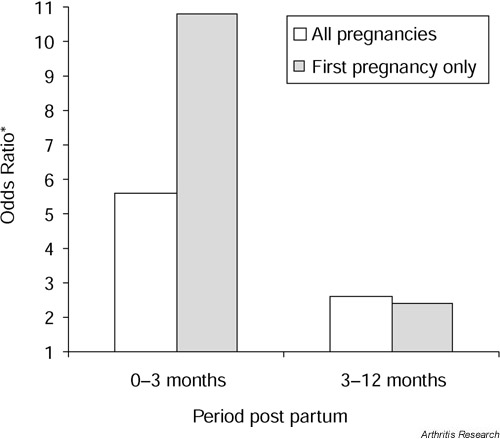
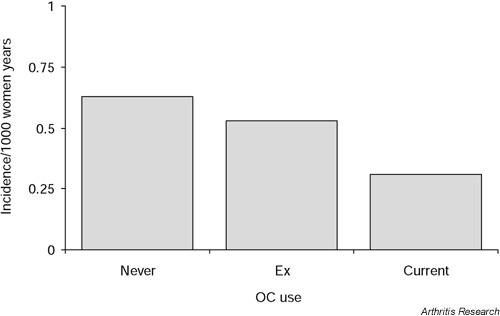
The prevalence of rheumatoid arthritis (RA) is relatively constant in many populations, at 0.5-1.0%. However, a high prevalence of RA has been reported in the Pima Indians (5.3%) and in the Chippewa Indians (6.8%). In contrast, low occurrences have been reported in populations from China and Japan. These data support a genetic role in disease risk. Studies have so far shown that the familial recurrence risk in RA is small compared with other autoimmune diseases. The main genetic risk factor of RA is the HLA DRB1 alleles, and this has consistently been shown in many populations throughout the world. The strongest susceptibility factor so far has been the HLA DRB1*0404 allele. Tumour necrosis factor alleles have also been linked with RA. However, it is estimated that these genes can explain only 50% of the genetic effect. A number of other non-MHC genes have thus been investigated and linked with RA (e.g. corticotrophin releasing hormone, oestrogen synthase, IFN-gamma and other cytokines). Environmental factors have also been studied in relation to RA. Female sex hormones may play a protective role in RA; for example, the use of the oral contraceptive pill and pregnancy are both associated with a decreased risk. However, the postpartum period has been highlighted as a risk period for the development of RA. Furthermore, breastfeeding after a first pregnancy poses the greatest risk. Exposure to infection may act as a trigger for RA, and a number of agents have been implicated (e.g. Epstein-Barr virus, parvovirus and some bacteria such as Proteus and Mycoplasma). However, the epidemiological data so far are inconclusive. There has recently been renewed interest in the link between cigarette smoking and RA, and the data presented so far are consistent with and suggestive of an increased risk.
类风湿关节炎(RA)在许多人群中的患病率相对稳定,为0.5%-1.0%。然而,据报道皮马印第安人(5.3%)和奇珀瓦印第安人(6.8%)中RA的患病率较高。相比之下,中国和日本人群中的发病率较低。这些数据支持了遗传因素在疾病风险中的作用。到目前为止的研究表明,与其他自身免疫性疾病相比,RA的家族复发风险较小。RA的主要遗传风险因素是HLA DRB1等位基因,这在全世界许多人群中都得到了一致证实。迄今为止最强的易感因素是HLA DRB1*0404等位基因。肿瘤坏死因子等位基因也与RA有关。然而,据估计这些基因只能解释50%的遗传效应。因此,人们对许多其他非MHC基因进行了研究,并将其与RA联系起来(例如促肾上腺皮质激素释放激素、雌激素合成酶、干扰素-γ和其他细胞因子)。环境因素也与RA有关。女性性激素可能在RA中起保护作用;例如,口服避孕药的使用和怀孕都与风险降低有关。然而,产后时期被认为是RA发病的风险期。此外,首次怀孕后的母乳喂养风险最大。接触感染可能是RA的触发因素,许多病原体都与此有关(例如爱泼斯坦-巴尔病毒、细小病毒以及一些细菌,如变形杆菌和支原体)。然而,目前的流行病学数据尚无定论。最近,人们对吸烟与RA之间的联系重新产生了兴趣,目前提供的数据表明两者之间存在关联,且提示吸烟会增加患病风险。