Lee J H, Suh G Y, Lee K Y, Yoo C G, Kim Y W, Han S K, Shim Y S, Kim K Y, Han Y C, Lee S D
Department of Internal Medicine, Seoul National University College of Medicine, Chungjoo, Korea.
Korean J Intern Med. 1992 Jul;7(2):87-93. doi: 10.3904/kjim.1992.7.2.87.
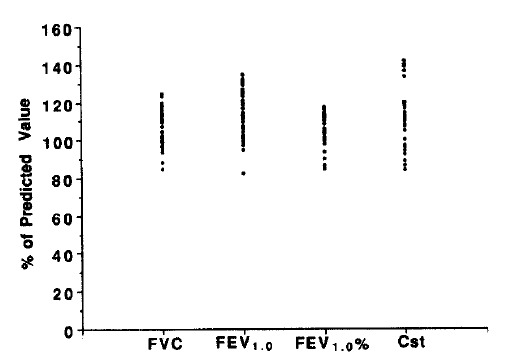
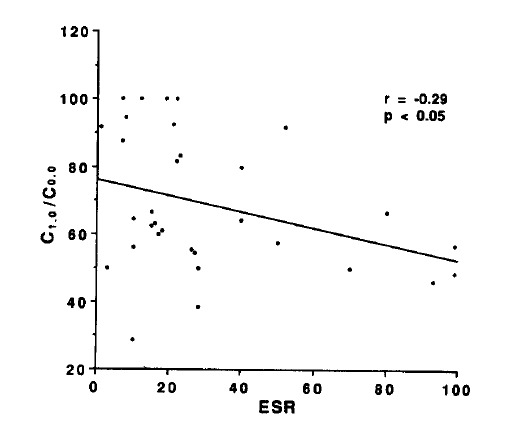
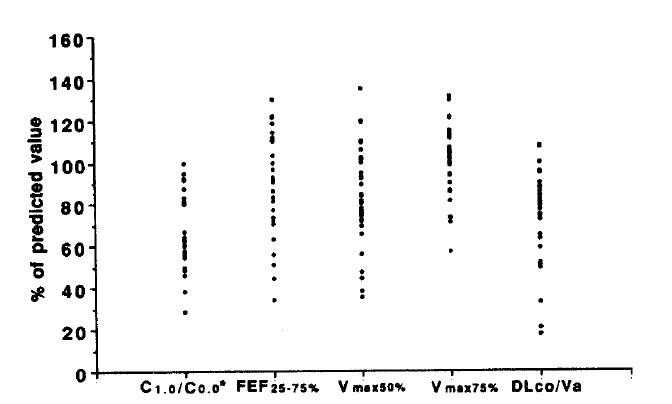
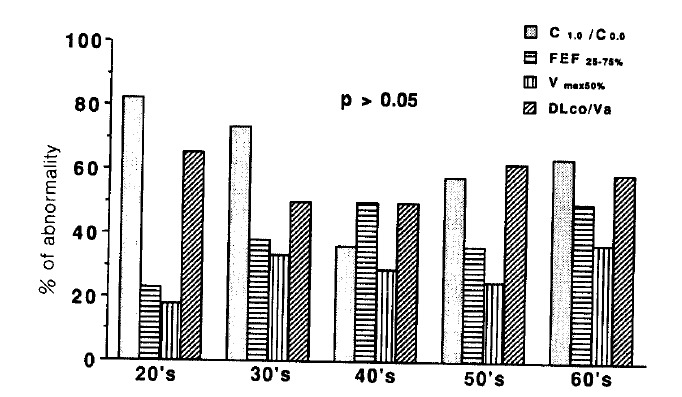
Variety of pulmonary lesions are thought to be associated with rheumatoid arthritis (RA). These lesions traditionally have included pleurisy with or without effusion, Caplan's syndrome, pulmonary rheumatoid nodules, diffuse interstitial fibrosis, and pulmonary arteritis and hypertension. But little attention has been paid to the airways in RA. Recently, several reports have suggested an association between airflow limitation and RA, but its incidence is not known. Also whether there exists a parameter of disease activity of RA, suggesting the presence of small airway disease (SAD) is not clear. To answer these questions, the serologic parameters which reflect the disease activity of RA and pulmonary function tests which reflect small airway dysfunction were performed on 36 lifetime nonsmokers with RA who had normal chest x-ray findings. The prevalence of SAD and the relationships between the disease activity parameters of RA and pulmonary function were observed. The results were as follows. The percentages of patients with abnormal values for diffusing capacity, frequency dependence of compliance (C1.0/C0.0), forced expiratory flow 25-75%, Vmax50% and Vmax 75% were 45.5%, 62.5%, 40%, 22.8% and 11.4%, respectively. There was statistically significant negative correlation between C1.0/C0.0 and ESR. But consistent correlation between other pulmonary function tests and clinical and serologic parameters of RA, and differences in pulmonary function between patients who were serologically positive and negative for CRP and FANA, were not found. In conclusion, SAD, without the influence of smoking, is frequently associated with RA, but the presence of SAD cannot be predicted from any clinical and serologic parameters of RA currently in use.
多种肺部病变被认为与类风湿关节炎(RA)相关。传统上,这些病变包括伴有或不伴有胸腔积液的胸膜炎、卡普兰综合征、肺部类风湿结节、弥漫性间质纤维化以及肺动脉炎和高血压。但RA患者的气道病变很少受到关注。最近,有几份报告提示气流受限与RA之间存在关联,但其发病率尚不清楚。此外,目前尚不清楚是否存在反映RA疾病活动的参数,提示小气道疾病(SAD)的存在。为回答这些问题,我们对36例胸部X线检查结果正常的终生不吸烟的RA患者进行了反映RA疾病活动的血清学参数和反映小气道功能障碍的肺功能测试。观察了SAD的患病率以及RA疾病活动参数与肺功能之间的关系。结果如下。弥散功能、顺应性频率依赖性(C1.0/C0.0)、用力呼气流量25%-75%、Vmax50%和Vmax75%异常的患者百分比分别为45.5%、62.5%、40%、22.8%和11.4%。C1.0/C0.0与血沉之间存在统计学显著的负相关。但未发现其他肺功能测试与RA的临床和血清学参数之间存在一致的相关性,以及C反应蛋白(CRP)和抗核抗体(FANA)血清学阳性和阴性患者之间的肺功能差异。总之,在无吸烟影响的情况下,SAD常与RA相关,但目前无法根据现有的RA临床和血清学参数预测SAD的存在。