Huwez F U, Pringle S D, Macfarlane P W
University Department of Medical Cardiology, Royal Infirmary, Glasgow.
Br Heart J. 1992 Apr;67(4):304-7. doi: 10.1136/hrt.67.4.304.
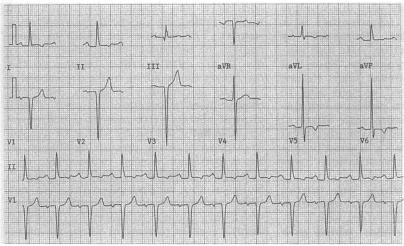
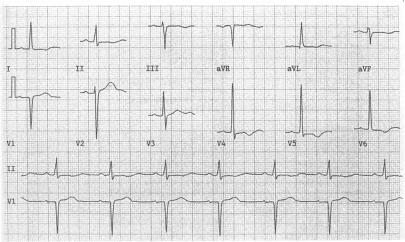
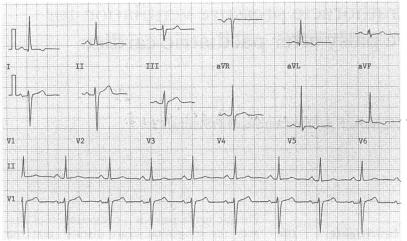
Classically, the ST-T configuration in the electrocardiogram of patients with left ventricular hypertrophy is said to have a typical pattern of ST depression together with asymmetrical T wave inversion (the so-called left ventricular strain pattern). However, many patients with left ventricular hypertrophy may also have ischaemic heart disease. To revise the electrocardiographic criteria for left ventricular hypertrophy the ST-T configuration in patients with left ventricular hypertrophy documented by echocardiography and with normal coronary arteries was assessed.
24 patients were selected for this study. All had left ventricular hypertrophy documented by echocardiography, normal coronary arteries by cardiac catheterisation, and ST and/or T wave abnormalities in the lateral leads of their electrocardiogram. There were eight patients with aortic valve disease and 16 with hypertension who had coronary angiography as part of an investigation into the risk factors of sudden cardiac death caused by hypertensive left ventricular hypertrophy. No patient was receiving digitalis preparations or had electrolyte disturbances, and none had a previous myocardial infarction or ventricular conduction defect.
Typical electrocardiographic evidence of left ventricular strain was found in approximately two thirds (63%) of patients and 95% of this subgroup had asymmetrical T wave inversion. Flat ST segment depression, with or without T wave inversion or isolated T wave inversion (symmetrical or asymmetrical) in the anterolateral leads, was seen in the remaining 37% of patients.
These findings indicate that left ventricular hypertrophy without coronary artery disease can cause variable types of ST-T abnormalities in the anterolateral leads including the typical left ventricular strain pattern and non-specific ST-T changes. Non-specific abnormalities could not be distinguished from those of coronary artery disease and may adversely affect the accuracy of the electrocardiographic criteria for the diagnosis of left ventricular hypertrophy because they do not accord with the criteria for left ventricular strain.
传统观点认为,左心室肥厚患者心电图的ST-T形态具有典型模式,即ST段压低伴不对称T波倒置(即所谓的左心室劳损图形)。然而,许多左心室肥厚患者也可能患有缺血性心脏病。为了修订左心室肥厚的心电图诊断标准,我们对经超声心动图证实为左心室肥厚且冠状动脉正常的患者的ST-T形态进行了评估。
本研究选取了24例患者。所有患者均经超声心动图证实有左心室肥厚,经心导管检查冠状动脉正常,且心电图侧导联有ST段和/或T波异常。其中8例患有主动脉瓣疾病,16例患有高血压,他们接受冠状动脉造影作为高血压性左心室肥厚所致心源性猝死危险因素调查的一部分。所有患者均未服用洋地黄制剂,无电解质紊乱,既往无心肌梗死或心室传导缺陷。
约三分之二(63%)的患者出现典型的左心室劳损心电图表现,该亚组中95%的患者有不对称T波倒置。其余37%的患者在前外侧导联可见ST段压低伴或不伴T波倒置或孤立的T波倒置(对称或不对称)。
这些发现表明,无冠状动脉疾病的左心室肥厚可导致前外侧导联出现多种类型的ST-T异常,包括典型的左心室劳损图形和非特异性ST-T改变。非特异性异常无法与冠状动脉疾病所致异常相区分,可能会对左心室肥厚心电图诊断标准的准确性产生不利影响,因为它们不符合左心室劳损的标准。