Holloway S, Porteous M, Cetnarskyj R, Anderson E, Rush R, Fry A, Gorman D, Steel M, Campbell H
Department of Clinical Genetics, Molecular Medicine Centre, Western General Hospital, Crewe Road South, Edinburgh EH4 2XU, UK.
Br J Cancer. 2004 Feb 9;90(3):582-9. doi: 10.1038/sj.bjc.6601562.
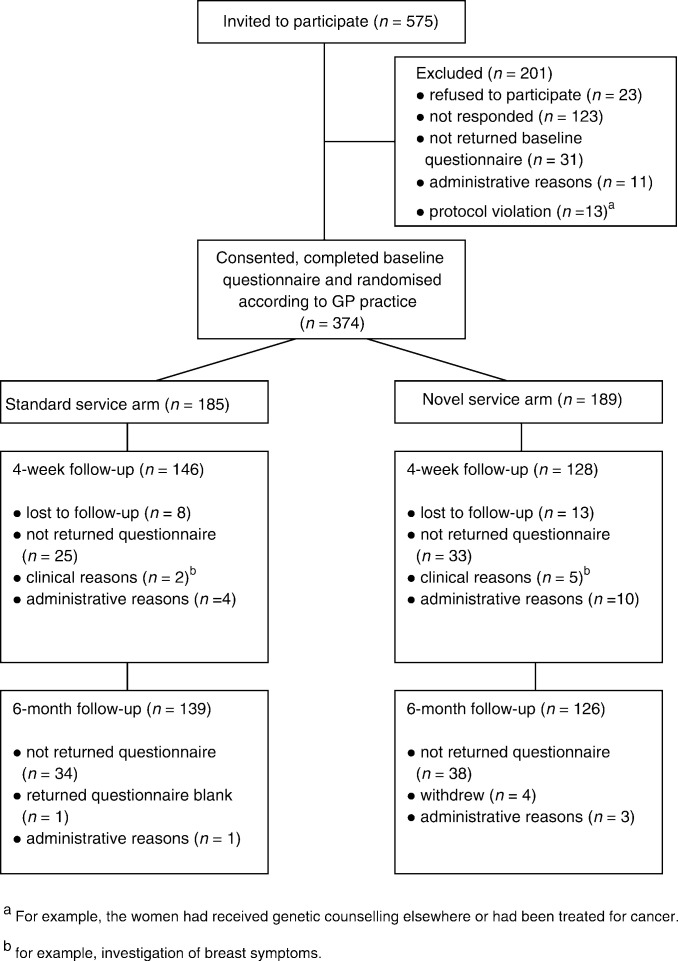
There is a need to integrate primary- and secondary-care cancer genetic services, but the most appropriate model of service delivery remains unclear. This study reports patients' expectations of breast cancer genetic services and a comparison of their satisfaction with two service models. In the first model, risk assessment was carried out using mailed family history data. Women estimated as being at high/moderate risk were offered an appointment at the familial breast cancer clinic, and those at low risk were sent a letter of reassurance. In the second model, all women were seen by a genetic nurse specialist, who assessed risk, referred high/moderate-risk women to the above clinic and discharged those at low risk. Over 60% of all women in the study regarded access to breast screening by mammogram and regular check-ups as very important. This underlines the demand for a multidisciplinary service providing both clinical genetic and surgical services. Satisfaction was high with both models of service, although significantly lower among women not at increased cancer risk and thus not offered a clinical check-up and mammography. Increased cancer worry was associated with a greater expressed need for information and for reassurance through follow-up clinical checks and mammography. Better targeting of counselling to the expressed concerns and needs of these women is required to improve the service offered. GPs and patients expressed no clear preference for any specific service location or staffing configuration. The novel community service was less expensive in terms of both staff and patient costs. The potential to decrease health staff/patient contact time and to employ nurse practitioners with both clinical genetic and oncology training should be explored further. The rapidly rising demand for these services suggests that the evaluation of further new models needs to continue to be given priority to guide the development of cancer genetic services.
整合初级和二级护理癌症基因服务很有必要,但最合适的服务提供模式仍不明确。本研究报告了患者对乳腺癌基因服务的期望,并比较了他们对两种服务模式的满意度。在第一种模式中,使用邮寄的家族病史数据进行风险评估。被估计为高/中度风险的女性会被安排在家族性乳腺癌诊所就诊,而低风险女性会收到一封安慰信。在第二种模式中,所有女性都由基因护士专家接诊,专家评估风险,将高/中度风险女性转诊至上述诊所,并让低风险女性出院。研究中超过60%的女性认为通过乳房X光检查进行乳房筛查和定期检查非常重要。这凸显了对提供临床基因和外科服务的多学科服务的需求。两种服务模式的满意度都很高,尽管在癌症风险未增加且因此未接受临床检查和乳房X光检查的女性中满意度明显较低。癌症担忧增加与通过后续临床检查和乳房X光检查表达出的对信息和安慰的更大需求相关。需要更好地针对这些女性表达的担忧和需求进行咨询,以改善所提供的服务。全科医生和患者对任何特定的服务地点或人员配置都没有明确偏好。新的社区服务在工作人员和患者成本方面都较低。应进一步探索减少医护人员/患者接触时间以及雇佣接受过临床基因和肿瘤学培训的执业护士的潜力。对这些服务迅速增长的需求表明,需要继续优先评估进一步的新模式,以指导癌症基因服务的发展。