Levitt David G
Department of Physiology, University of Minnesota, Minneapolis, U.S.A.
BMC Clin Pharmacol. 2004 Feb 19;4:2. doi: 10.1186/1472-6904-4-2.
Modeling of pharmacokinetic parameters and pharmacodynamic actions requires knowledge of the arterial blood concentration. In most cases, experimental measurements are only available for a peripheral vein (usually antecubital) whose concentration may differ significantly from both arterial and central vein concentration.
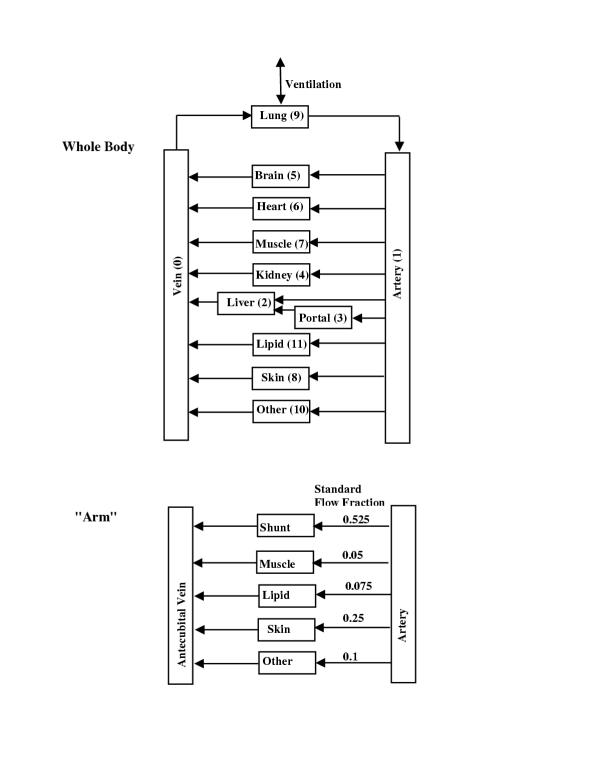
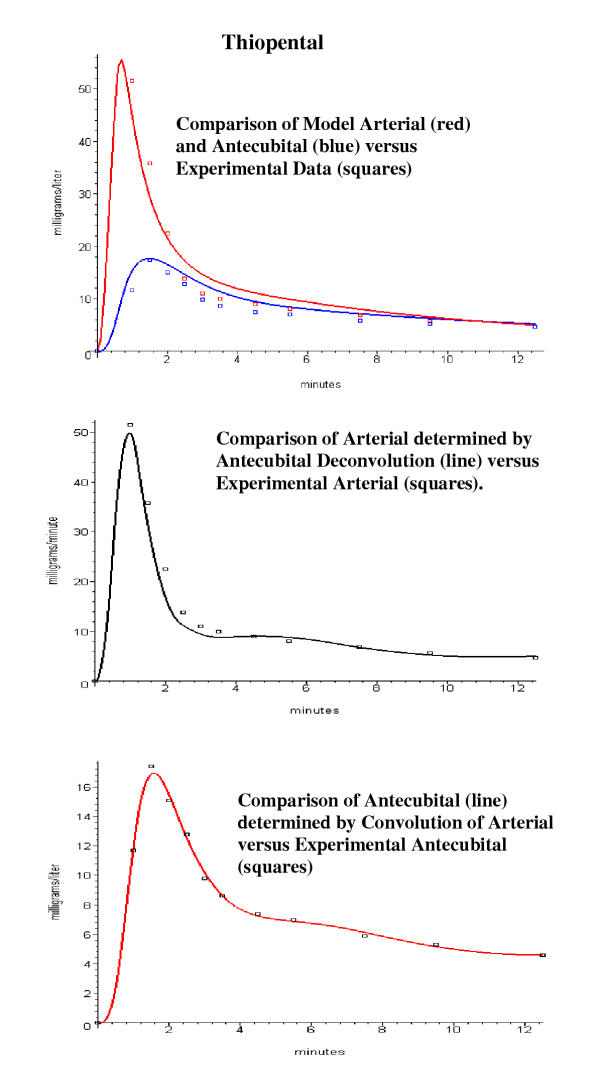
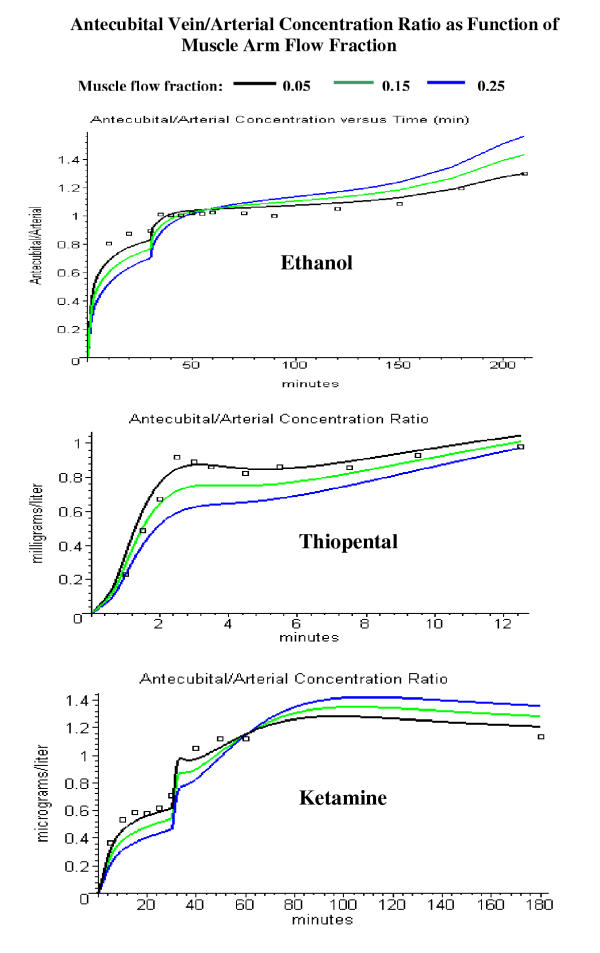
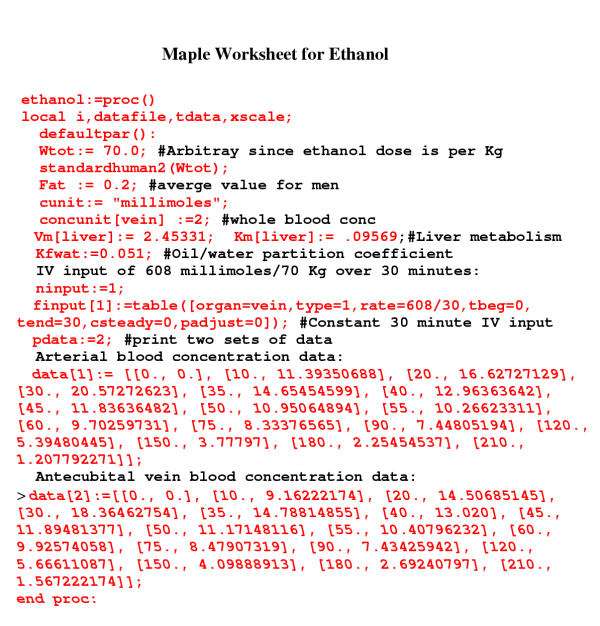
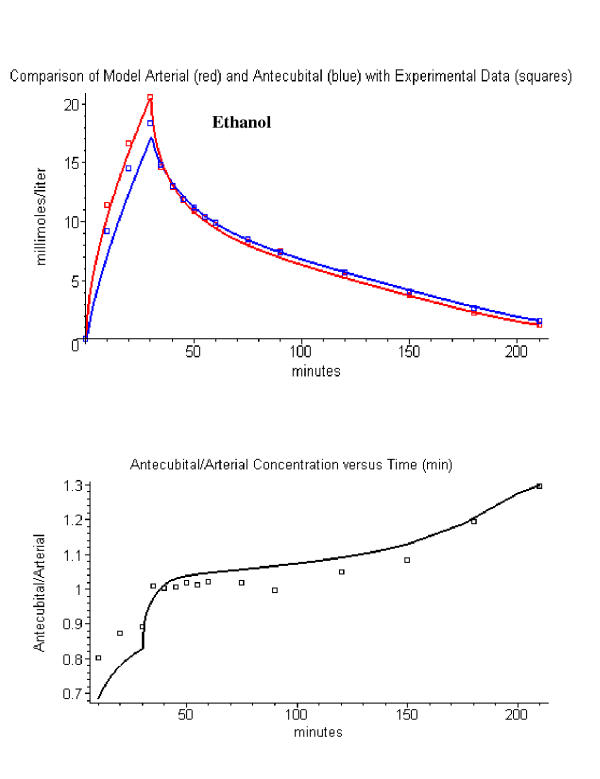
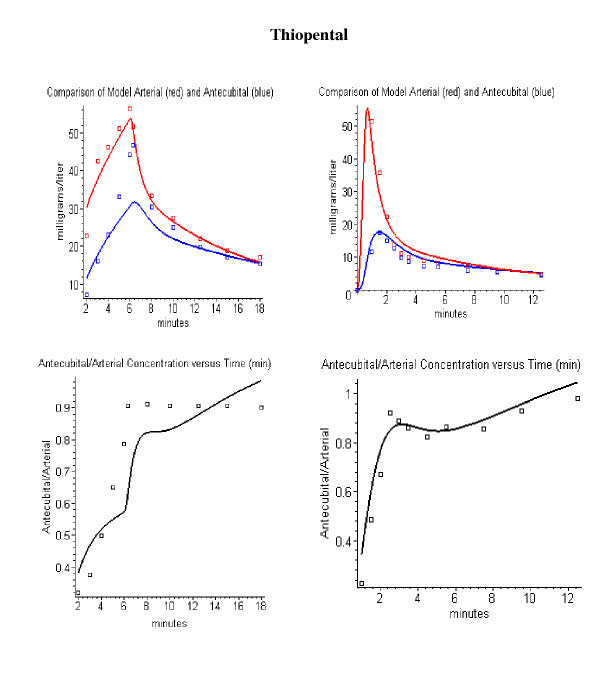
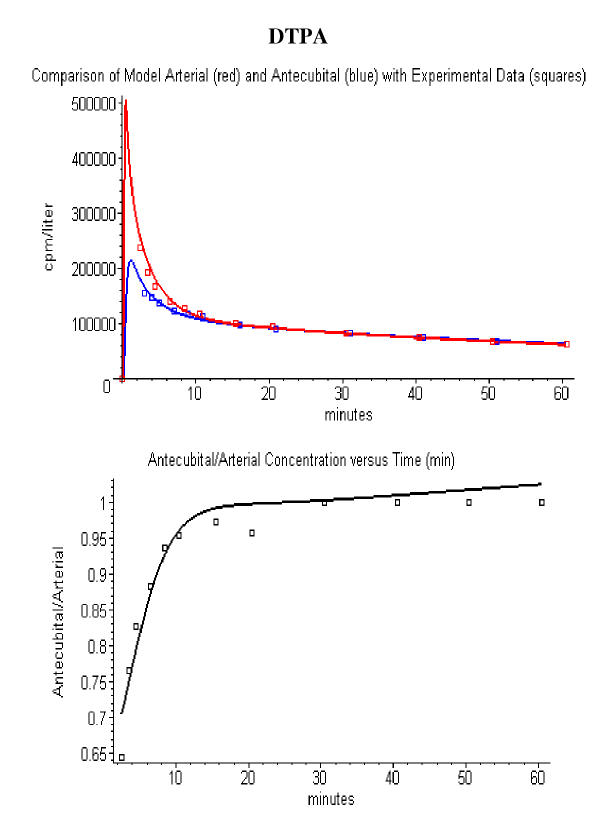
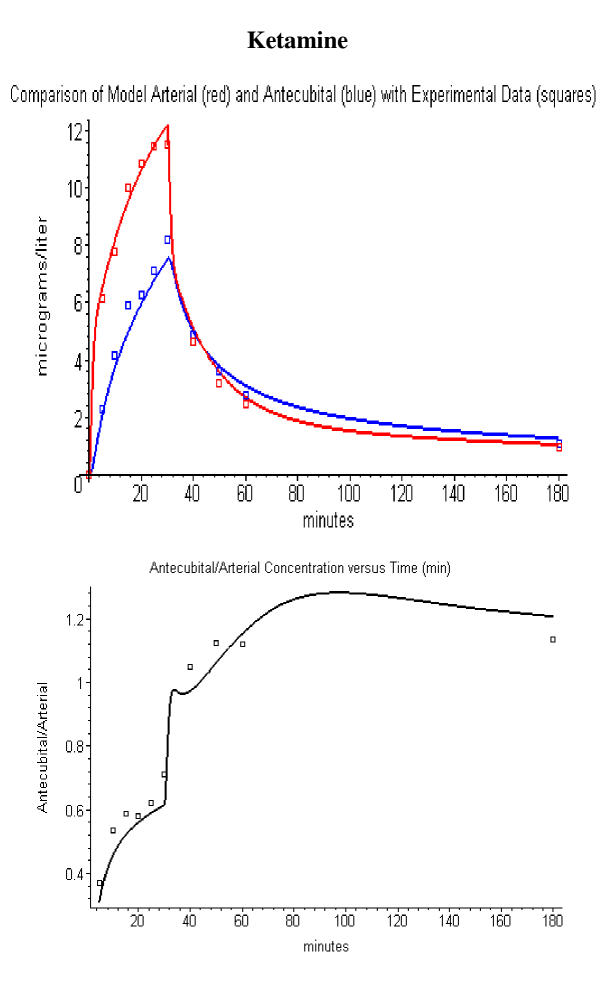
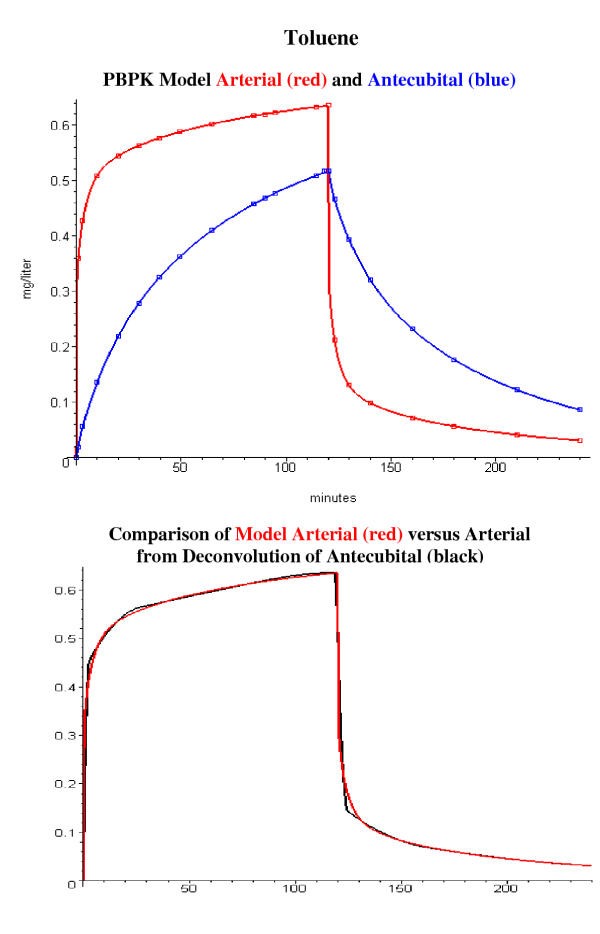
A physiologically based pharmacokinetic (PBPK) model for the tissues drained by the antecubital vein (referred to as "arm") is developed. It is assumed that the "arm" is composed of tissues with identical properties (partition coefficient, blood flow/gm) as the whole body tissues plus a new "tissue" representing skin arteriovenous shunts. The antecubital vein concentration depends on the following parameters: the fraction of "arm" blood flow contributed by muscle, skin, adipose, connective tissue and arteriovenous shunts, and the flow per gram of the arteriovenous shunt. The value of these parameters was investigated using simultaneous experimental measurements of arterial and antecubital concentrations for eight solutes: ethanol, thiopental, 99Tcm-diethylene triamine pentaacetate (DTPA), ketamine, D2O, acetone, methylene chloride and toluene. A new procedure is described that can be used to determine the arterial concentration for an arbitrary solute by deconvolution of the antecubital concentration. These procedures are implemented in PKQuest, a general PBPK program that is freely distributed http://www.pkquest.com.
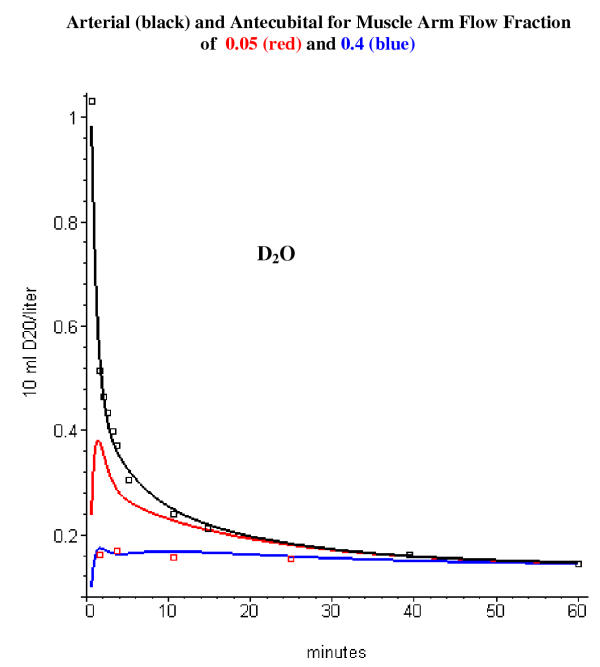
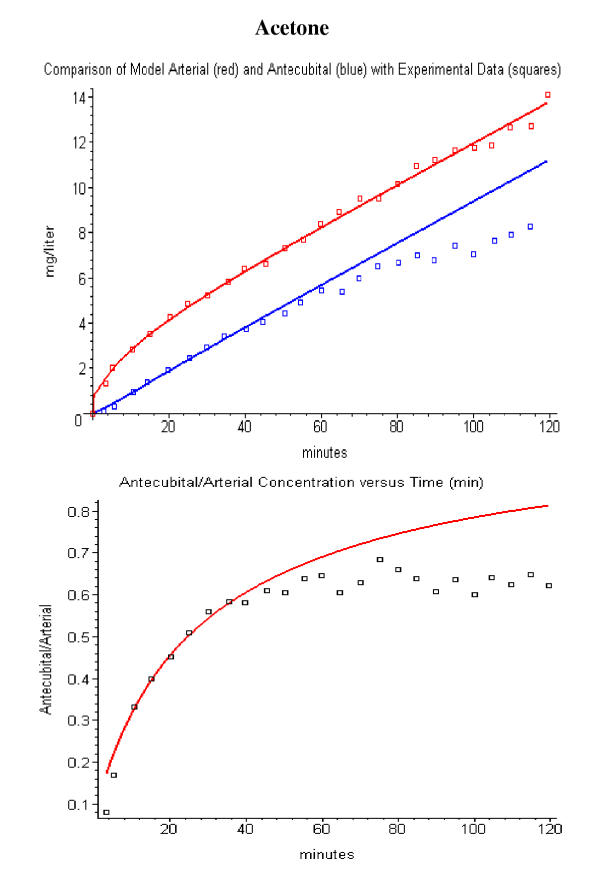
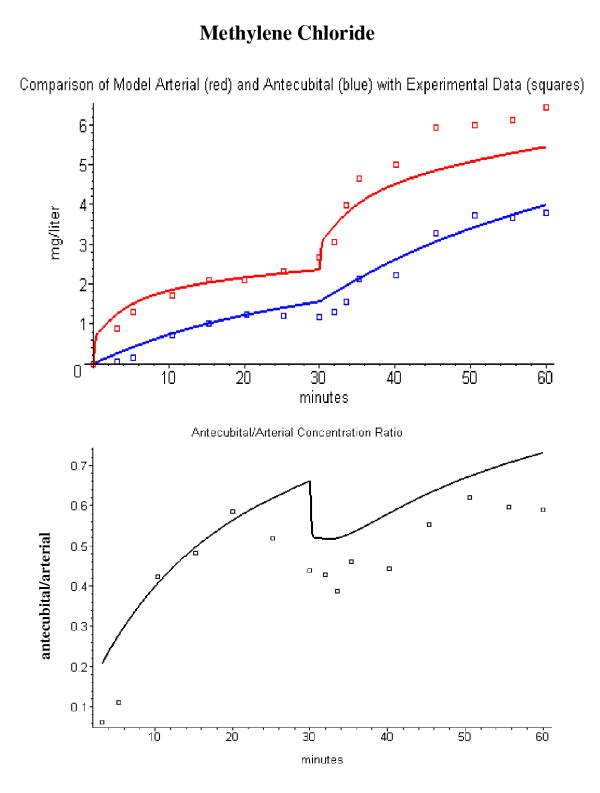
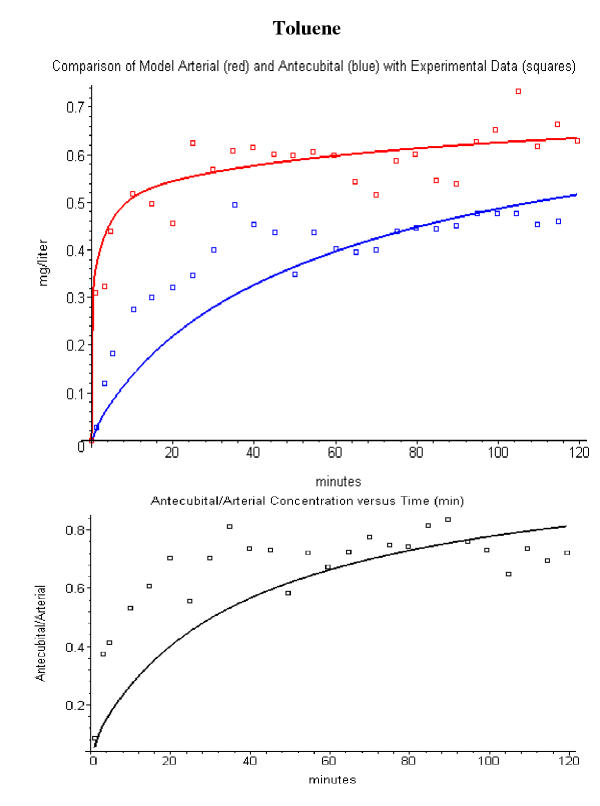
One set of "standard arm" parameters provides an adequate description of the arterial/antecubital vein concentration for ethanol, DTPA, thiopental and ketamine. A significantly different set of "arm" parameters was required to describe the data for D2O, acetone, methylene chloride and toluene - probably because the "arm" is in a different physiological state.
Using the set of "standard arm" parameters, the antecubital vein concentration can be used to determine the whole body PBPK model parameters for an arbitrary solute without any additional adjustable parameters. Also, the antecubital vein concentration can be used to estimate the arterial concentration for an arbitrary input for solutes for which no arterial concentration data is available.
药代动力学参数和药效学作用的建模需要动脉血浓度的相关知识。在大多数情况下,实验测量仅能获取外周静脉(通常为肘前静脉)的浓度,而该浓度可能与动脉和中心静脉浓度存在显著差异。
构建了一个基于生理学的药代动力学(PBPK)模型,用于模拟肘前静脉引流的组织(称为“手臂”)。假定“手臂”由与全身组织具有相同性质(分配系数、每克血流量)的组织以及代表皮肤动静脉分流的新“组织”组成。肘前静脉浓度取决于以下参数:肌肉、皮肤、脂肪、结缔组织和动静脉分流对“手臂”血流量的贡献比例,以及每克动静脉分流的血流量。使用八种溶质(乙醇、硫喷妥钠、99锝-二乙三胺五乙酸(DTPA)、氯胺酮、重水、丙酮、二氯甲烷和甲苯)的动脉和肘前浓度的同步实验测量数据,对这些参数的值进行了研究。描述了一种新方法,可通过对肘前浓度进行反卷积来确定任意溶质的动脉浓度。这些方法在PKQuest中得以实现,PKQuest是一个可免费从http://www.pkquest.com获取的通用PBPK程序。
一组“标准手臂”参数能够充分描述乙醇、DTPA、硫喷妥钠和氯胺酮的动脉/肘前静脉浓度。描述重水、丙酮、二氯甲烷和甲苯的数据则需要一组显著不同的“手臂”参数——这可能是因为“手臂”处于不同的生理状态。
使用“标准手臂”参数集,肘前静脉浓度可用于确定任意溶质的全身PBPK模型参数,而无需任何额外的可调参数。此外,对于没有动脉浓度数据的溶质,肘前静脉浓度可用于估计任意输入时的动脉浓度。