Balarajan R, Yuen P, Machin D
Institute of Public Health, University of Surrey, Guildford.
BMJ. 1992 Feb 29;304(6826):529-34. doi: 10.1136/bmj.304.6826.529.
To examine general practitioner consultations by demographic and socioeconomic variables and to derive a method of measuring the impact of relative deprivation on general practitioner workload.
The study was based on general practitioner consultations reported in the general household surveys of 1983-7, covering a sample of 129,987 individuals in Great Britain. Odds ratios for general practitioner consultations were obtained for selected variables among children (0-15 years), men (16-64), women (16-64), and elderly people (greater than or equal to 65). These were then used to derive deprivation indices specific to electoral wards for use in general practice.
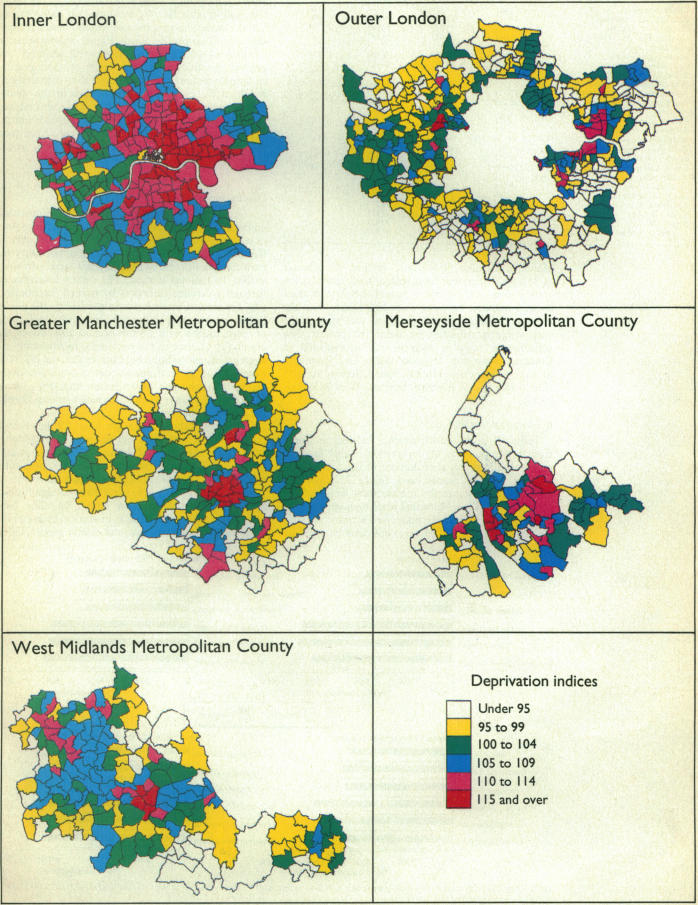
Great Britain, with particular findings illustrated by English electoral wards and the conurbations of London, Manchester, Merseyside, and the West Midlands.
Council tenure increased the likelihood of consultation significantly in all four groups. Odds ratios were raised in children, men, and women with no access to a car. Birth in the New Commonwealth or Pakistan yielded high odds ratios in men, women, and elderly people but not in children. Marginally increased consultation rates were evident in the manual socioeconomic groups in women, elderly people, and children with a single parent mother. The deprivation indices for general practice derived using these odds ratios varied substantially among English electoral wards with, for example, anticipated general practitioner consultations in the electoral ward of Hulme, Manchester, being 24% higher than the average ward in England as a result of local attributes, and consultations in the Cheam South ward of Sutton, London, 11% lower than average.
This deprivation index for general practice overcomes several shortcomings expressed about the underprivileged area score, which has been adopted in the 1990 contract as a basis for allocating deprivation supplements to general practitioners. The proposed index can be applied nationwide.
根据人口统计学和社会经济变量研究全科医生诊疗情况,并得出一种衡量相对贫困对全科医生工作量影响的方法。
本研究基于1983 - 1987年全国家庭调查中报告的全科医生诊疗情况,涵盖英国129,987名个体样本。获取了儿童(0 - 15岁)、男性(16 - 64岁)、女性(16 - 64岁)和老年人(≥65岁)中选定变量的全科医生诊疗比值比。然后将这些比值比用于得出特定选区的贫困指数,以供全科医疗使用。
英国,以英格兰选区以及伦敦、曼彻斯特、默西塞德郡和西米德兰兹郡的城区的具体研究结果为例。
在所有四个群体中,市政任期显著增加了诊疗的可能性。没有汽车的儿童、男性和女性的比值比升高。出生在英联邦新成员国或巴基斯坦的男性、女性和老年人的比值比很高,但儿童中并非如此。在女性、老年人以及母亲为单亲的儿童的体力劳动者社会经济群体中,诊疗率略有上升。使用这些比值比得出的全科医疗贫困指数在英格兰选区之间差异很大,例如,由于当地特征,曼彻斯特胡尔姆选区预计的全科医生诊疗比英格兰平均选区高24%,而伦敦萨顿的切姆南区的诊疗比平均水平低11%。
这种全科医疗贫困指数克服了对弱势群体区域得分所表达的几个缺点,1990年的合同采用该得分作为向全科医生分配贫困补贴的基础。所提议的指数可在全国范围内应用。