Kim Seung Kwon, Lim Hyo K, Ryu Jeong-ah, Choi Dongil, Lee Won Jae, Lee Ji Yeon, Lee Ju Hyun, Sung Yon Mi, Cho Eun Yoon, Hong Seung-Mo, Kim Jong-Sung
Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Kangnam-gu, Seoul, Korea.
Korean J Radiol. 2004 Oct-Dec;5(4):240-9. doi: 10.3348/kjr.2004.5.4.240.
We wished to evaluate the effect of the Pringle maneuver (occlusion of both the hepatic artery and portal vein) on the pathologic changes in the hepatic vessels, bile ducts and liver parenchyma surrounding the ablation zone in rabbit livers.
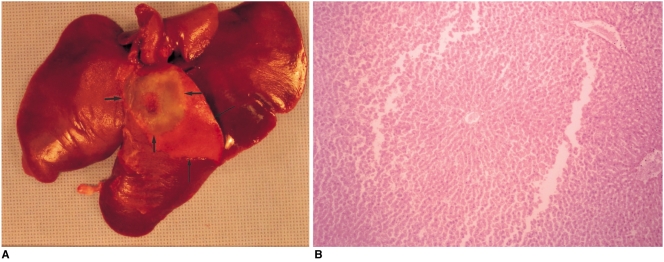
Radiofrequency (RF) ablation zones were created in the livers of 24 rabbits in vivo by using a 50-W, 480-kHz monopolar RF generator and a 15-gauge expandable electrode with four sharp prongs for 7 mins. The tips of the electrodes were placed in the liver parenchyma near the porta hepatis with the distal 1 cm of their prongs deployed. Radiofrequency ablation was performed in the groups with (n=12 rabbits) and without (n=12 rabbits) the Pringle maneuver. Three animals of each group were sacrificed immediately, three days (the acute phase), seven days (the early subacute phase) and two weeks (the late subacute phase) after RF ablation. The ablation zones were excised and serial pathologic changes in the hepatic vessels, bile ducts and liver parenchyma surrounding the ablation zone were evaluated.
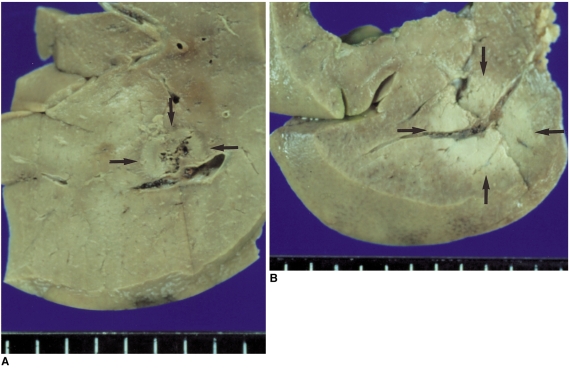
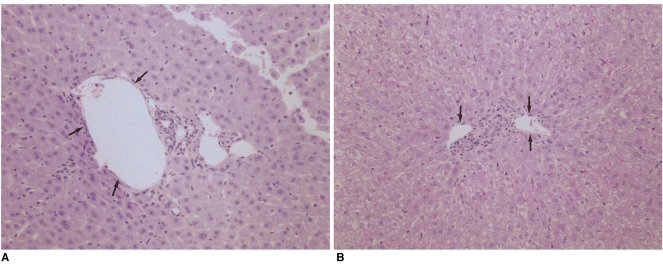
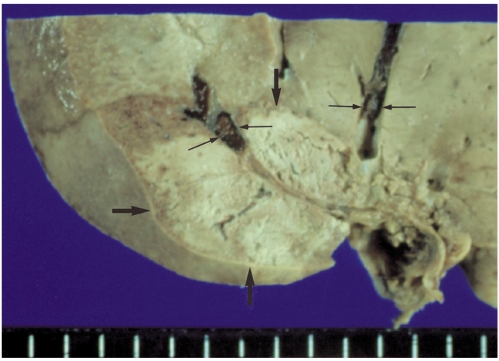
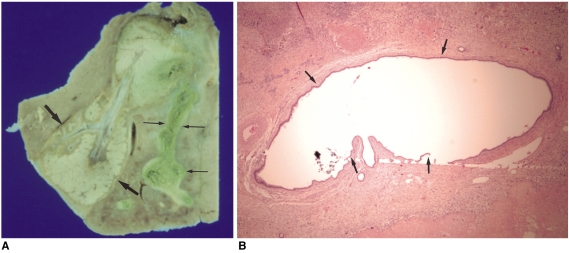
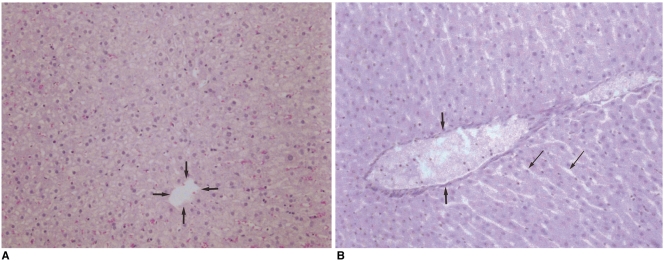
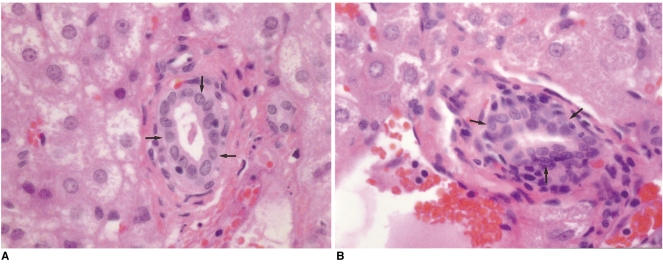
With the Pringle maneuver, portal vein thrombosis was found in three cases (in the immediate [n=2] and acute phase [n=1]), bile duct dilatation adjacent to the ablation zone was found in one case (in the late subacute phase [n=1]), infarction adjacent to the ablation zone was found in three cases (in the early subacute [n=2] and late subacute [n=1] phases). None of the above changes was found in the livers ablated without the Pringle maneuver. On the microscopic findings, centrilobular congestion, sinusoidal congestion, sinusoidal platelet and neutrophilic adhesion, and hepatocyte vacuolar and ballooning changes in liver ablated with Pringle maneuver showed more significant changes than in those livers ablated without the Pringle maneuver (p < 0.05)
Radiofrequency ablation with the Pringle maneuver created more severe pathologic changes in the portal vein, bile ducts and liver parenchyma surrounding the ablation zone compared with RF ablation without the Pringle maneuver. Therefore, we suggest that RF ablation with the Pringle maneuver should be performed with great caution in order to avoid unwanted thermal injury.
我们希望评估普林格尔手法(阻断肝动脉和门静脉)对兔肝脏消融区周围肝血管、胆管及肝实质病理变化的影响。
使用50W、480kHz单极射频发生器及带有四个尖锐叉头的15号可扩张电极,在24只兔肝脏内制造射频(RF)消融区,持续7分钟。将电极尖端置于肝门附近的肝实质内,使叉头远端1cm展开。对实施普林格尔手法的组(n = 12只兔)和未实施普林格尔手法的组(n = 12只兔)进行射频消融。每组三只动物在射频消融后立即、三天(急性期)、七天(早期亚急性期)和两周(晚期亚急性期)处死。切除消融区,评估消融区周围肝血管、胆管及肝实质的系列病理变化。
采用普林格尔手法时,发现3例门静脉血栓形成(即时[n = 2]和急性期[n = 1]),1例消融区附近胆管扩张(晚期亚急性期[n = 1]),3例消融区附近梗死(早期亚急性期[n = 2]和晚期亚急性期[n = 1])。未采用普林格尔手法消融的肝脏未发现上述变化。显微镜检查发现,采用普林格尔手法消融的肝脏中央小叶充血、窦状隙充血、窦状隙血小板和中性粒细胞黏附以及肝细胞空泡化和气球样变比未采用普林格尔手法消融的肝脏更明显(p < 0.05)。
与未采用普林格尔手法的射频消融相比,采用普林格尔手法的射频消融在消融区周围门静脉、胆管及肝实质产生更严重的病理变化。因此,我们建议采用普林格尔手法的射频消融应谨慎进行,以避免不必要的热损伤。