Feresu Shingairai A, Harlow Siobán D, Welch Kathy, Gillespie Brenda W
Department of Preventive and Societal Medicine, University of Nebraska Medical Center 984350 Nebraska Medical Center, Omaha, NE 68198-4350, USA.
BMC Pregnancy Childbirth. 2005 May 5;5(1):9. doi: 10.1186/1471-2393-5-9.
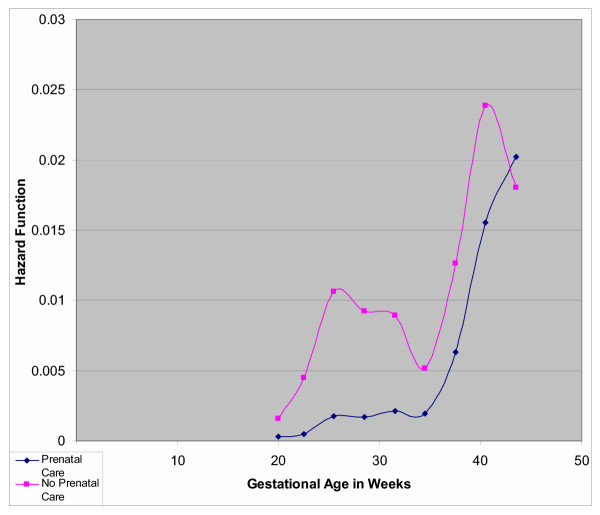
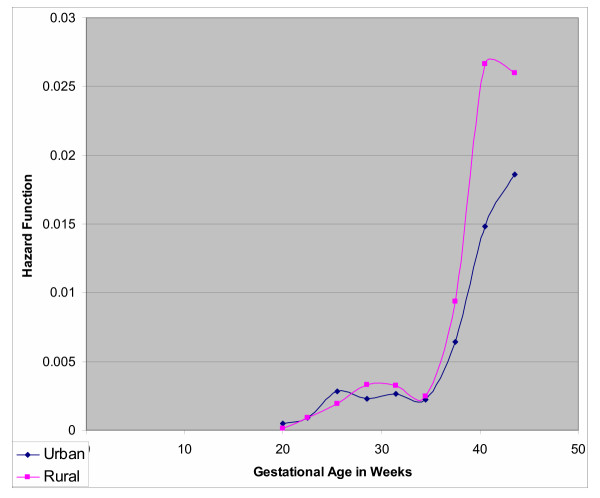
Death of an infant in utero or at birth has always been a devastating experience for the mother and of concern in clinical practice. Infant mortality remains a challenge in the care of pregnant women worldwide, but particularly for developing countries and the need to understand contributory factors is crucial for addressing appropriate perinatal health. METHODS: Using information available in obstetric records for all deliveries (17,072 births) at Harare Maternity Hospital, Zimbabwe, we conducted a cross-sectional retrospective analysis of a one-year data, (1997-1998) to assess demographic and obstetric risk factors for stillbirth and early neonatal death. We estimated risk of stillbirth and early neonatal death for each potential risk factor. RESULTS: The annual frequency of stillbirth was 56 per 1,000 total births. Women delivering stillbirths and early neonatal deaths were less likely to receive prenatal care (adjusted relative risk [RR] = 2.54; 95% confidence intervals [CI] 2.19-2.94 and RR = 2.52; 95% CI 1.63-3.91), which for combined stillbirths and early neonatal deaths increased with increasing gestational age (Hazard Ratio [HR] = 3.98, HR = 7.49 at 28 and 40 weeks of gestation, respectively). Rural residence was associated with risk of infant dying in utero, (RR = 1.33; 95% CI 1.12-1.59), and the risk of death increased with increasing gestational age (HR = 1.04, HR = 1.69, at 28 and 40 weeks of gestation, respectively). Older maternal age was associated with risk of death (HR = 1.50; 95% CI 1.21-1.84). Stillbirths were less likely to be delivered by Cesarean section (RR = 0.64; 95% CI 0.51-0.79), but more likely to be delivered as breech (RR = 4.65; 95% CI 3.88-5.57, as were early neonatal deaths (RR = 3.38; 95% CI 1.64-6.96). CONCLUSION: The frequency of stillbirth, especially macerated, is high, 27 per 1000 total births. Early prenatal care could help reduce perinatal death linking the woman to the health care system, increasing the probability that she would seek timely emergency care that would reduce the likelihood of death of her infant in utero. Improved quality of obstetric care during labor and delivery may help reduce the number of fresh stillbirths and early neonatal deaths.
子宫内或出生时婴儿死亡对母亲来说一直是毁灭性的经历,也是临床实践中关注的问题。婴儿死亡率在全球孕妇护理中仍然是一项挑战,尤其是在发展中国家,了解促成因素对于解决适当的围产期健康问题至关重要。
利用津巴布韦哈拉雷妇产医院所有分娩(17072例出生)的产科记录中的可用信息,我们对一年(1997 - 1998年)的数据进行了横断面回顾性分析,以评估死产和早期新生儿死亡的人口统计学和产科风险因素。我们估计了每个潜在风险因素的死产和早期新生儿死亡风险。
死产的年发生率为每1000例总出生数中有56例。分娩死产和早期新生儿死亡的妇女接受产前护理的可能性较小(调整后的相对风险[RR]=2.54;95%置信区间[CI]2.19 - 2.94,RR = 2.52;95%CI 1.63 - 3.91),对于合并的死产和早期新生儿死亡,随着孕周增加而增加(风险比[HR]=3.98,在妊娠28周和40周时HR分别为7.49)。农村居住与子宫内婴儿死亡风险相关(RR = 1.33;95%CI 1.12 - 1.59),且死亡风险随着孕周增加而增加(在妊娠28周和40周时HR分别为1.04和1.69)。母亲年龄较大与死亡风险相关(HR = 1.50;95%CI 1.21 - 1.84)。死产通过剖宫产分娩的可能性较小(RR = 0.64;95%CI 0.51 - 0.79),但更有可能以臀位分娩(RR = 4.65;95%CI 3.88 - 5.57),早期新生儿死亡也是如此(RR = 3.38;95%CI 1.64 - 6.96)。
死产的发生率很高,尤其是浸软死产,每1000例总出生数中有27例。早期产前护理有助于降低围产期死亡,将妇女与医疗保健系统联系起来,增加她寻求及时急诊护理的可能性,从而降低子宫内婴儿死亡的可能性。分娩期间和分娩时改善产科护理质量可能有助于减少新鲜死产和早期新生儿死亡的数量。