Yorke Ellen, Rosenzweig Kenneth E, Wagman Raquel, Mageras Gikas S
Department of Medical Physics, Memorial Sloan Kettering Cancer Center, 1275 York Avenue, New York City, New York 10021, USA.
J Appl Clin Med Phys. 2005 Spring;6(2):19-32. doi: 10.1120/jacmp.v6i2.2048. Epub 2005 May 19.
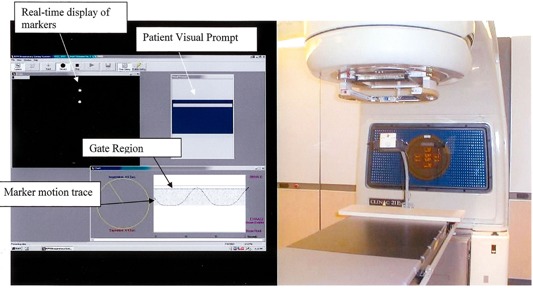
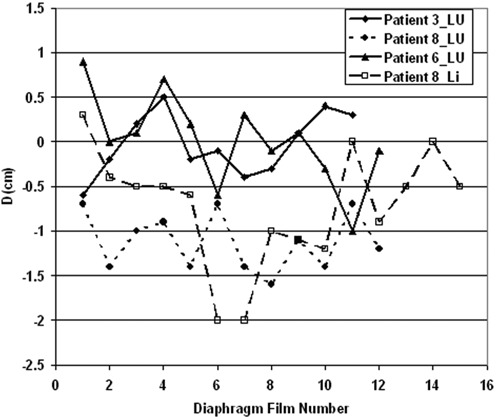
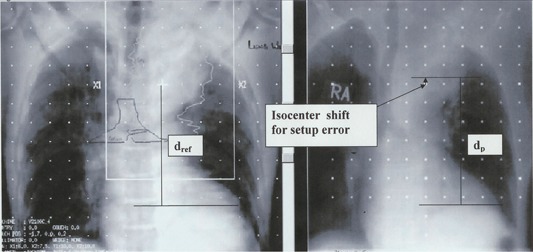
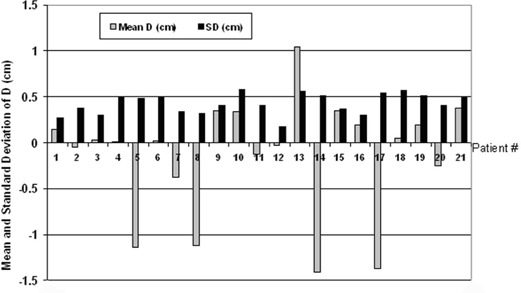
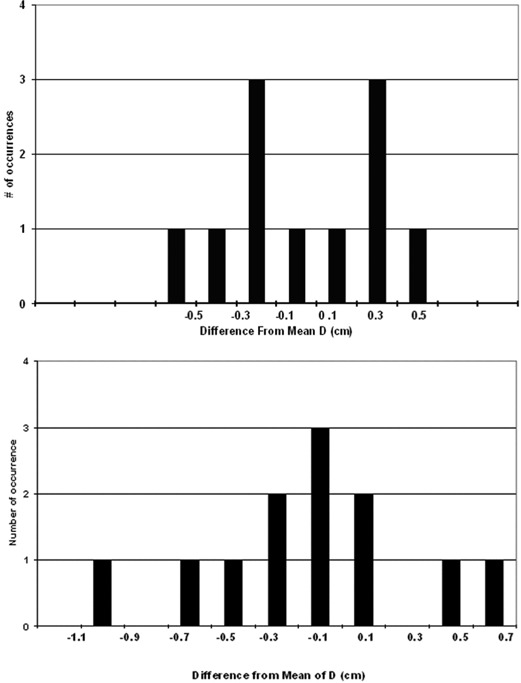
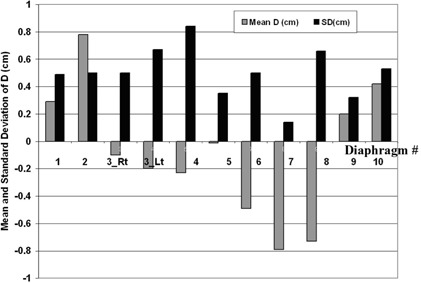
As quality assurance for respiration-gated treatments using the Varian RPM system, we monitor interfractional diaphragm variation throughout treatment using extra anterior-posterior (AP) portal images. We measure the superior-inferior (SI distance between one or more bony landmarks and the ipsilateral diaphragm dome in each such radiograph and calculate its difference, D, from the corresponding distance in a planning CT scan digitally reconstructed radiograph (DRR). For each patient, the mean of D represents the systematic diaphragm displacement, and the standard deviation of D represents random diaphragm variations and is a measure of interfractional gating reproducibility. We present results for 31 sequential patients (21 lung, 10 liver tumors), each with at least 8 such portal images. For all patients, the gate included end-exhale. The patient-specific duty cycle ranged from 30% to 60%. All patients received customized audio prompting for simulation and treatment, and 14 patients also received visual prompting. Respiration-synchronized fluoroscopic movies taken at a conventional simulator revealed patient-specific diaphragm excursions from 1.0 cm to 5.0 cm and diaphragm excursion within the gate from 0.5 cm to 1.0 cm, demonstrating a significant reduction of intra-fractional diaphragm (and by inference tumor) motion by respiratory gating. One standard deviation of the systematic displacement (the mean of D) was 0.63 cm and 0.48 cm for the lung and liver patient groups, respectively. The average +/-1 SD of the random displacements (i.e., the average of the standard deviations of D) was 0.42 +/- 0.11 cm and 0.50 +/- 0.19 for the two groups, respectively. The similar magnitude of the systematic and random displacements suggests that both derive from a common distribution of interfractional variations. Combining visual with audio prompting did not significantly improve performance, as judged by D. Guided by these portal images, field changes were made during the course of treatment for 6 patients (1 lung, 5 liver).
作为使用瓦里安RPM系统进行呼吸门控治疗的质量保证措施,我们在整个治疗过程中利用额外的前后(AP)射野图像监测分次治疗间的膈肌变化。我们在每张此类射线照片中测量一个或多个骨性标志与同侧膈肌穹窿之间的上下(SI)距离,并计算其与计划CT扫描数字重建射线照片(DRR)中相应距离的差值D。对于每位患者,D的平均值代表膈肌的系统位移,D的标准差代表膈肌的随机变化,是分次治疗间门控重复性的一种度量。我们给出了31例连续患者(21例肺癌、10例肝癌)的结果,每位患者至少有8张此类射野图像。对于所有患者,门控包括呼气末。患者特定的工作周期范围为30%至60%。所有患者在模拟和治疗过程中均接受定制的音频提示,14例患者还接受了视觉提示。在传统模拟器上拍摄的呼吸同步透视电影显示,患者特定的膈肌移动范围为1.0厘米至5.0厘米,门控内的膈肌移动范围为0.5厘米至1.0厘米,表明呼吸门控显著减少了分次治疗内膈肌(进而推断肿瘤)的运动。肺癌和肝癌患者组系统位移的一个标准差(D的平均值)分别为0.63厘米和0.48厘米。两组随机位移的平均±1标准差(即D的标准差的平均值)分别为0.42±0.11厘米和0.50±0.19厘米。系统位移和随机位移的幅度相似,表明两者均源自分次治疗间变化的共同分布。根据D判断,视觉提示与音频提示相结合并未显著改善性能。在这些射野图像的指导下,6例患者(1例肺癌、5例肝癌)在治疗过程中进行了射野调整。