Nazarian Saman, Bluemke David A, Lardo Albert C, Zviman Menekhem M, Watkins Stanley P, Dickfeld Timm L, Meininger Glenn R, Roguin Ariel, Calkins Hugh, Tomaselli Gordon F, Weiss Robert G, Berger Ronald D, Lima João A C, Halperin Henry R
Department of Medicine/Cardiology, Johns Hopkins Hospital, Baltimore, MD 21287, USA.
Circulation. 2005 Nov 1;112(18):2821-5. doi: 10.1161/CIRCULATIONAHA.105.549659.
Patients with left ventricular dysfunction have an elevated risk of sudden cardiac death. However, the substrate for ventricular arrhythmia in patients with nonischemic cardiomyopathy remains poorly understood. We hypothesized that the distribution of scar identified by MRI is predictive of inducible ventricular tachycardia.
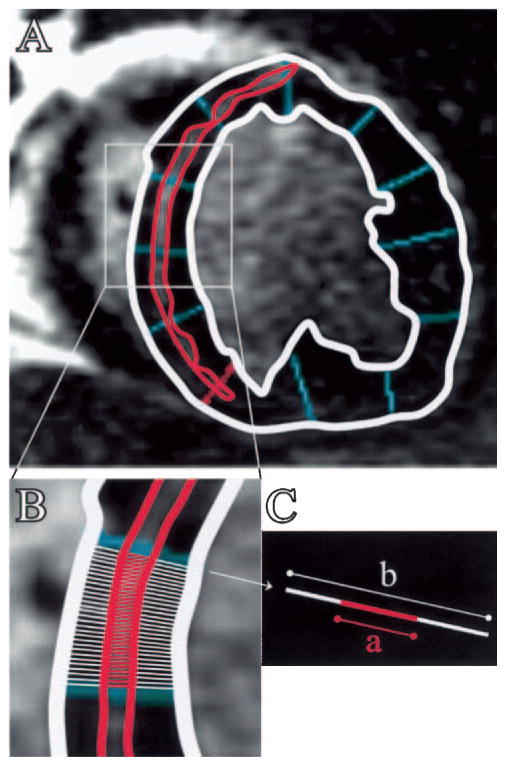
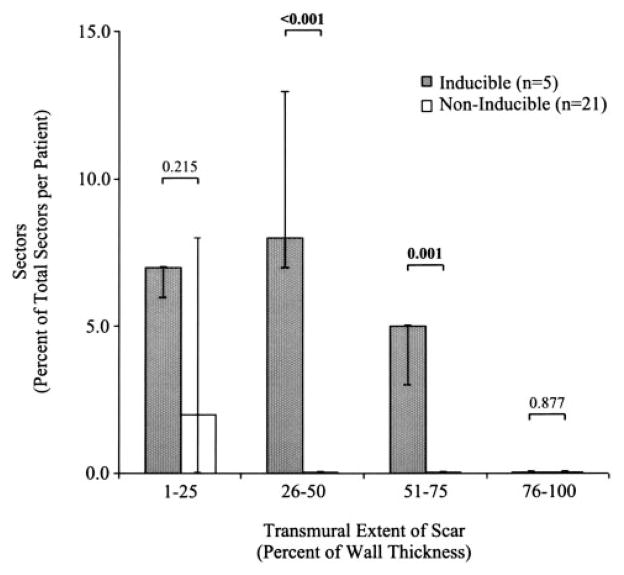
Short-axis cine steady-state free-precession and postcontrast inversion-recovery gradient-echo MRI sequences were obtained before electrophysiological study in 26 patients with nonischemic cardiomyopathy. Left ventricular ejection fraction was measured from end-diastolic and end-systolic cine images. The transmural extent of scar as a percentage of wall thickness (percent scar transmurality) in each of 12 radial sectors per slice was calculated in all myocardial slices. The percentages of sectors with 1% to 25%, 26% to 50%, 51% to 75%, and 76% to 100% scar transmurality were determined for each patient. Predominance of scar distribution involving 26% to 75% of wall thickness was significantly predictive of inducible ventricular tachycardia and remained independently predictive in the multivariable model after adjustment for left ventricular ejection fraction (odds ratio, 9.125; P=0.020).
MR assessment of scar distribution can identify the substrate for inducible ventricular tachycardia and may identify high-risk patients with nonischemic cardiomyopathy currently missed by ejection fraction criteria.
左心室功能不全患者发生心源性猝死的风险升高。然而,非缺血性心肌病患者室性心律失常的基质仍了解甚少。我们假设磁共振成像(MRI)识别出的瘢痕分布可预测可诱导的室性心动过速。
在对26例非缺血性心肌病患者进行电生理研究之前,获取短轴电影稳态自由进动序列和对比剂增强后反转恢复梯度回波MRI序列。从舒张末期和收缩末期电影图像测量左心室射血分数。计算每一层心肌中12个径向节段中每个节段瘢痕透壁范围占壁厚的百分比(瘢痕透壁百分比)。确定每位患者瘢痕透壁百分比为1%至25%、26%至50%、51%至75%和76%至100%的节段百分比。瘢痕分布占壁厚26%至75%具有显著预测可诱导室性心动过速的作用,在调整左心室射血分数后的多变量模型中仍具有独立预测作用(优势比,9.125;P = 0.020)。
MRI对瘢痕分布的评估可识别可诱导室性心动过速的基质,并可能识别出目前根据射血分数标准遗漏的非缺血性心肌病高危患者。