Macario Alex, Chow John L, Dexter Franklin
Department of Anesthesia, Stanford University School of Medicine, Stanford, CA 94305, USA.
BMC Med Inform Decis Mak. 2006 Mar 15;6:15. doi: 10.1186/1472-6947-6-15.
Management of acute respiratory distress syndrome (ARDS) in the intensive care unit (ICU) is clinically challenging and costly. Neuromuscular blocking agents may facilitate mechanical ventilation and improve oxygenation, but may result in prolonged recovery of neuromuscular function and acute quadriplegic myopathy syndrome (AQMS). The goal of this study was to address a hypothetical question via computer modeling: Would a reduction in intubation time of 6 hours and/or a reduction in the incidence of AQMS from 25% to 21%, provide enough benefit to justify a drug with an additional expenditure of $267 (the difference in acquisition cost between a generic and brand name neuromuscular blocker)?
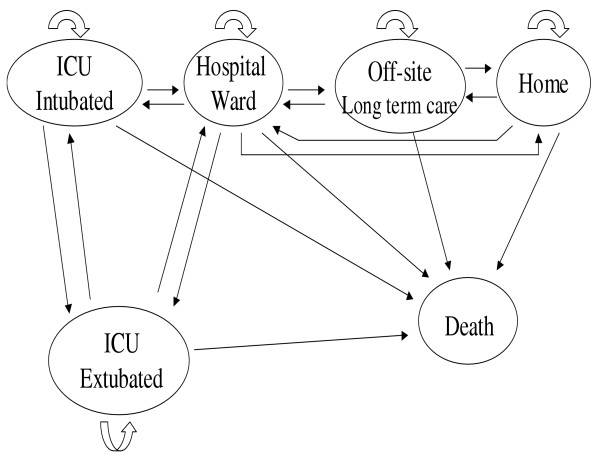
The base case was a 55 year-old man in the ICU with ARDS who receives neuromuscular blockade for 3.5 days. A Markov model was designed with hypothetical patients in 1 of 6 mutually exclusive health states: ICU-intubated, ICU-extubated, hospital ward, long-term care, home, or death, over a period of 6 months. The net monetary benefit was computed.
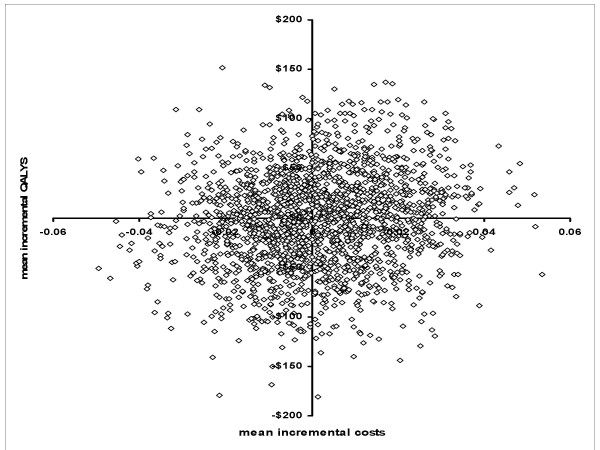
Our computer simulation modeling predicted the mean cost for ARDS patients receiving standard care for 6 months to be $62,238 (5%-95% percentiles $42,259-$83,766), with an overall 6-month mortality of 39%. Assuming a ceiling ratio of $35,000, even if a drug (that cost $267 more) hypothetically reduced AQMS from 25% to 21% and decreased intubation time by 6 hours, the net monetary benefit would only equal $137.
ARDS patients receiving a neuromuscular blocker have a high mortality, and unpredictable outcome, which results in large variability in costs per case. If a patient dies, there is no benefit to any drug that reduces ventilation time or AQMS incidence. A prospective, randomized pharmacoeconomic study of neuromuscular blockers in the ICU to asses AQMS or intubation times is impractical because of the highly variable clinical course of patients with ARDS.
重症监护病房(ICU)中急性呼吸窘迫综合征(ARDS)的管理在临床上具有挑战性且成本高昂。神经肌肉阻滞剂可能有助于机械通气并改善氧合,但可能导致神经肌肉功能恢复延长和急性四肢瘫性肌病综合征(AQMS)。本研究的目的是通过计算机建模解决一个假设性问题:插管时间减少6小时和/或AQMS发生率从25%降至21%,是否能带来足够的益处,以证明使用一种额外花费267美元的药物是合理的(通用型和品牌型神经肌肉阻滞剂采购成本的差异)?
基础病例是一名55岁的ICU中患有ARDS的男性,接受神经肌肉阻滞3.5天。设计了一个马尔可夫模型,假设有6种相互排斥的健康状态之一的患者:ICU插管、ICU拔管、医院病房、长期护理、家庭或死亡,为期6个月。计算净货币效益。
我们的计算机模拟模型预测,接受标准护理6个月的ARDS患者的平均成本为62,238美元(5% - 95%百分位数为42,259 - 83,766美元),总体6个月死亡率为39%。假设上限比率为35,000美元,即使一种药物(成本高出267美元)假设将AQMS从25%降至21%并将插管时间减少6小时,净货币效益也仅为137美元。
接受神经肌肉阻滞剂治疗的ARDS患者死亡率高且预后不可预测,这导致每个病例的成本差异很大。如果患者死亡,任何减少通气时间或AQMS发生率的药物都没有益处。由于ARDS患者的临床病程高度可变,对ICU中神经肌肉阻滞剂进行前瞻性、随机药物经济学研究以评估AQMS或插管时间是不切实际