George S, Primrose J, Talbot R, Smith J, Mullee M, Bailey D, du Boulay C, Jordan H
Public Health Sciences and Medical Statistics, Southampton General Hospital, University of Southampton, Mailpoint 805, Tremona Road, Southampton SO16 6YD, UK.
Br J Cancer. 2006 Oct 9;95(7):841-7. doi: 10.1038/sj.bjc.6603352. Epub 2006 Sep 12.
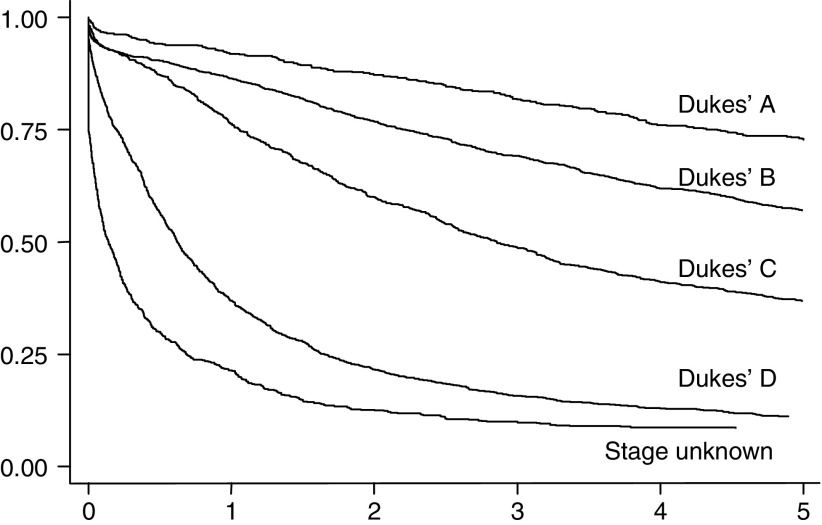
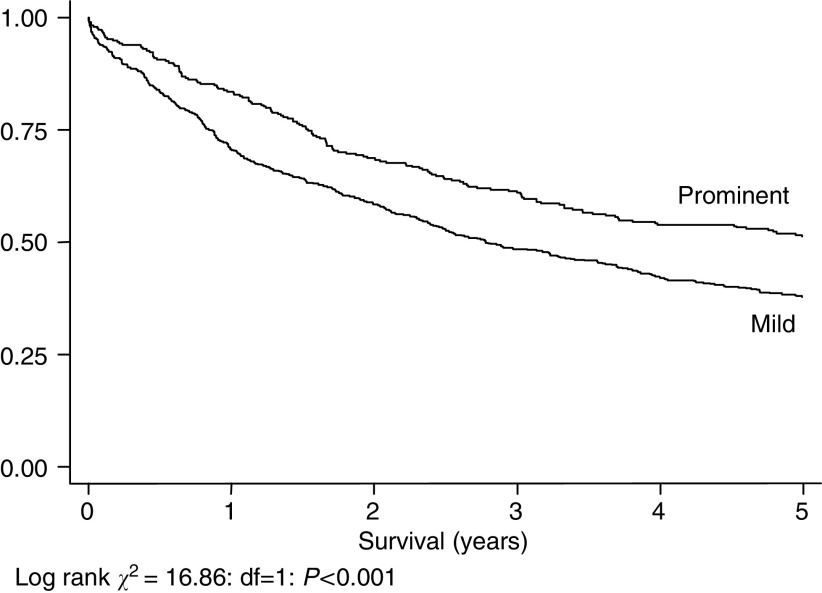
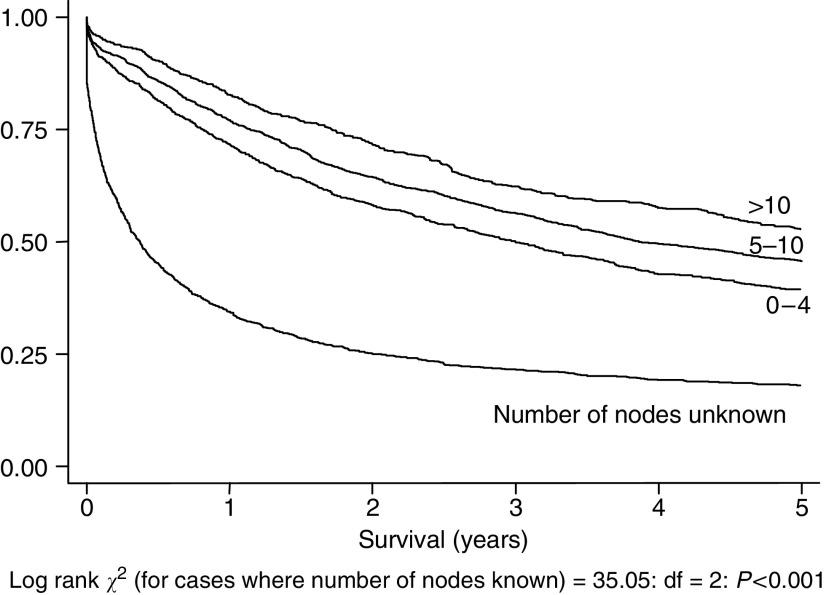
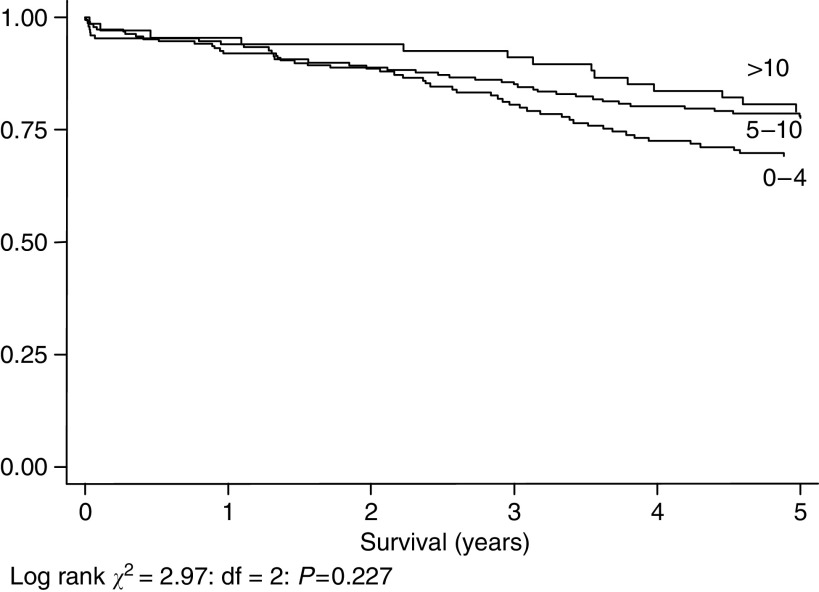
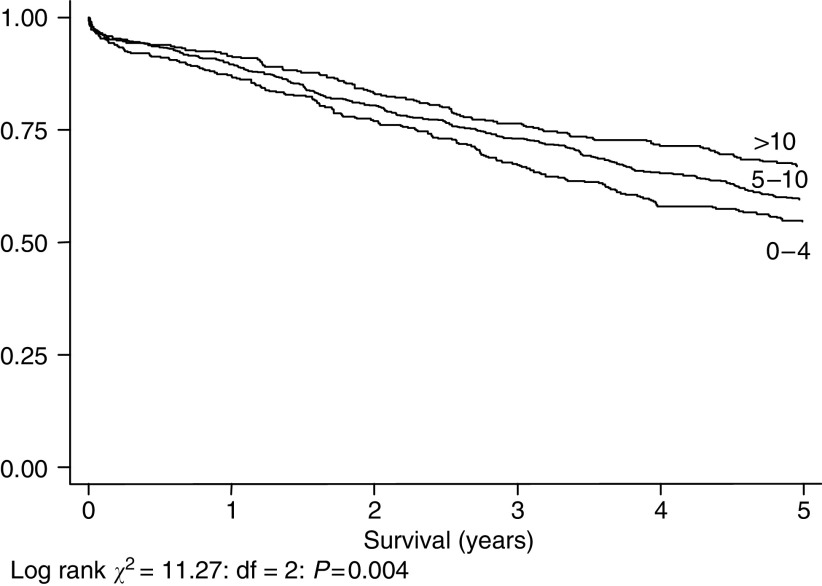
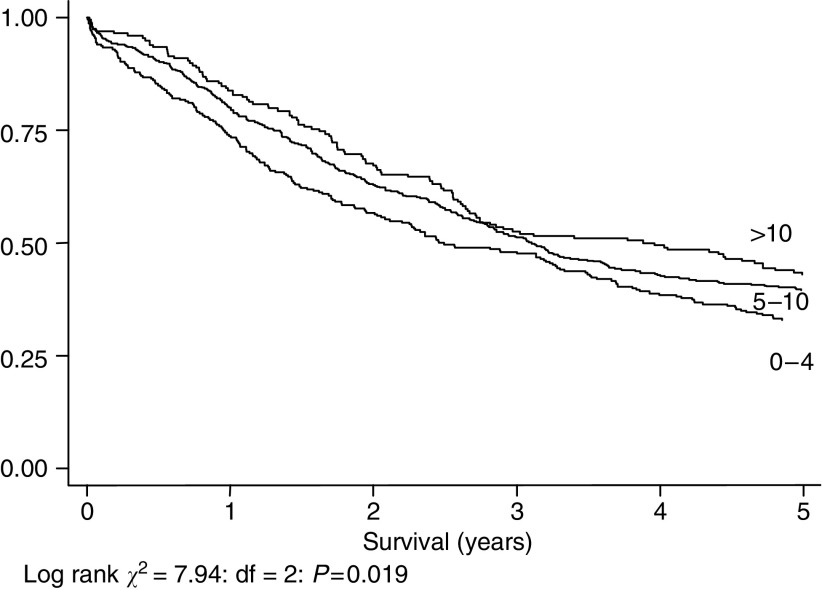
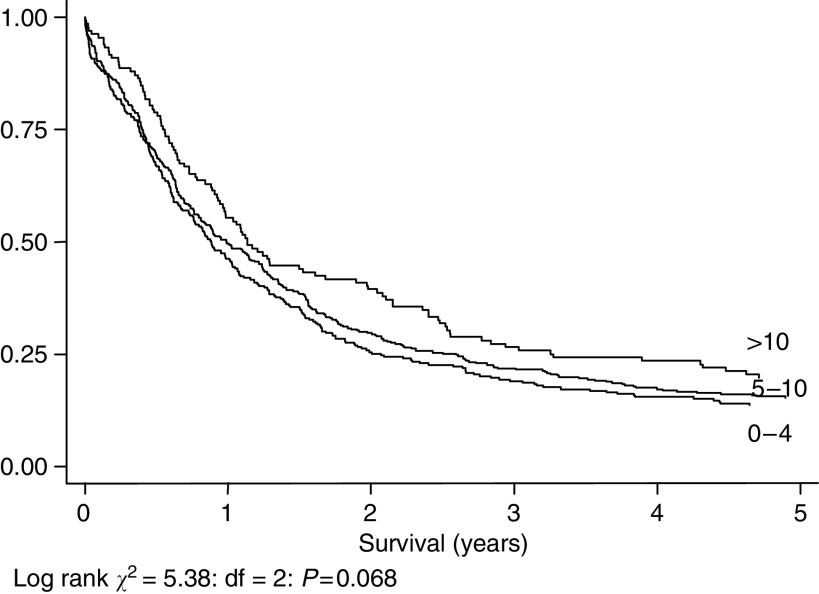
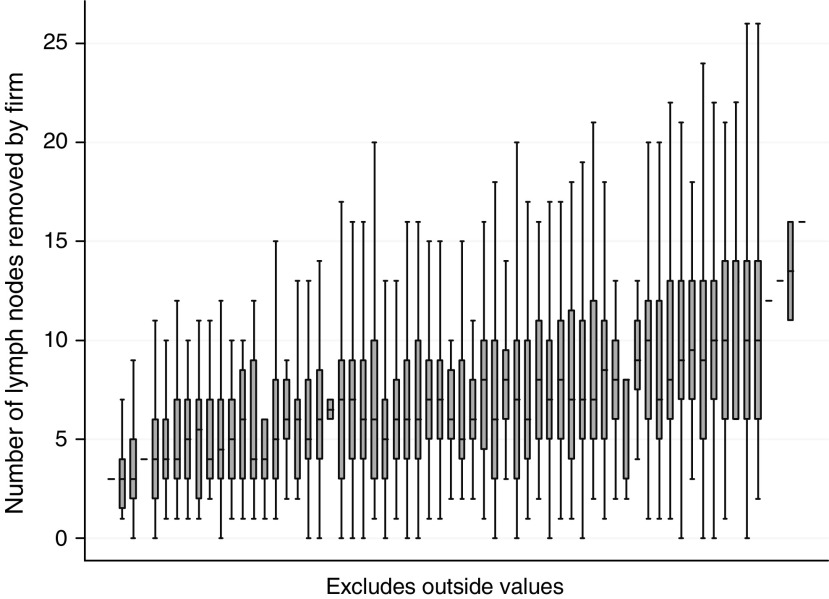
To investigate the relationship between survival in colorectal cancer patients and the number of lymph nodes examined by a pathologist, previously attributed to stage migration, we used data from a cohort of 5174 colorectal cancer patients recruited between September 1991 and August 1994, and followed-up for 5 years. We selected cases with data present on all prognostic variables, and stratified them into three groups by number of nodes examined. We made a multivariate survival comparison using a Cox regression model. In all, there were 3592 cases with data present on all prognostic variables. Patients who had >10 nodes identified had a significant survival advantage over those who had 5-10 identified, who had in turn a similar advantage over those with 0-4 identified (P<0.001). This effect was present in the whole group and at all Dukes' stages, although statistically significant only in stages B (P=0.004) and C (P=0.019). The effect remained after adjustment in a Cox regression model in which the mean number of nodes taken out by each surgical firm did not predict survival. In a sub-group with data on lymphocytic infiltration into the primary tumour a survival advantage was noted in those with prominent rather than mild infiltration (P<0.001): the former also tended to have more nodes found (P=0.015). Stage migration alone cannot explain these results, as survival advantages are noted across the whole population independent of stage. Lymphocytic infiltration into the primary tumour is prognostically important, and is associated with the number of nodes found. Reactive enlargement of lymph nodes in the mesentery may make them easier to find, reflect immune response to the tumour, and thus indirectly impact upon survival.
为了研究结直肠癌患者的生存率与病理学家检查的淋巴结数量之间的关系(此前认为这归因于分期迁移),我们使用了1991年9月至1994年8月招募的5174例结直肠癌患者的数据,并进行了5年的随访。我们选择了所有预后变量数据完整的病例,并根据检查的淋巴结数量将其分为三组。我们使用Cox回归模型进行多变量生存比较。总共有3592例病例所有预后变量数据完整。发现淋巴结>10个的患者比发现5 - 10个淋巴结的患者有显著的生存优势,而后者又比发现0 - 4个淋巴结的患者有类似优势(P<0.001)。这种效应在整个组以及所有Dukes分期中均存在,尽管仅在B期(P = 0.004)和C期(P = 0.019)有统计学意义。在调整Cox回归模型后,这种效应仍然存在,在该模型中每个外科团队取出的淋巴结平均数量并不能预测生存率。在一个有原发性肿瘤淋巴细胞浸润数据的亚组中,发现浸润显著而非轻度的患者有生存优势(P<0.001):前者发现的淋巴结也往往更多(P = 0.015)。仅分期迁移无法解释这些结果,因为在整个群体中无论分期如何都能观察到生存优势。原发性肿瘤中的淋巴细胞浸润具有预后重要性,并且与发现的淋巴结数量相关。肠系膜淋巴结的反应性增大可能使其更容易被发现,反映对肿瘤的免疫反应,从而间接影响生存率。