Escombe A Roderick, Oeser Clarissa C, Gilman Robert H, Navincopa Marcos, Ticona Eduardo, Pan William, Martínez Carlos, Chacaltana Jesus, Rodríguez Richard, Moore David A J, Friedland Jon S, Evans Carlton A
Department of Infectious Diseases & Immunity, Imperial College London, London, United Kingdom.
PLoS Med. 2007 Feb;4(2):e68. doi: 10.1371/journal.pmed.0040068.
Institutional transmission of airborne infections such as tuberculosis (TB) is an important public health problem, especially in resource-limited settings where protective measures such as negative-pressure isolation rooms are difficult to implement. Natural ventilation may offer a low-cost alternative. Our objective was to investigate the rates, determinants, and effects of natural ventilation in health care settings.
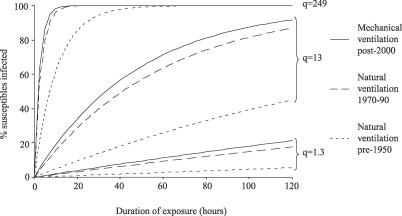
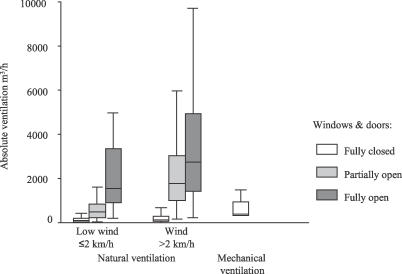
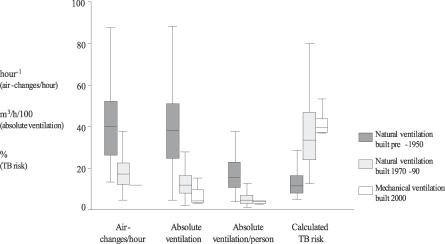
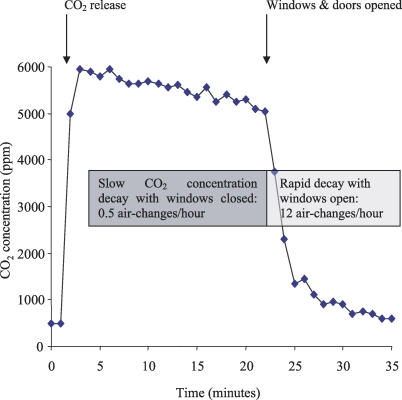
The study was carried out in eight hospitals in Lima, Peru; five were hospitals of "old-fashioned" design built pre-1950, and three of "modern" design, built 1970-1990. In these hospitals 70 naturally ventilated clinical rooms where infectious patients are likely to be encountered were studied. These included respiratory isolation rooms, TB wards, respiratory wards, general medical wards, outpatient consulting rooms, waiting rooms, and emergency departments. These rooms were compared with 12 mechanically ventilated negative-pressure respiratory isolation rooms built post-2000. Ventilation was measured using a carbon dioxide tracer gas technique in 368 experiments. Architectural and environmental variables were measured. For each experiment, infection risk was estimated for TB exposure using the Wells-Riley model of airborne infection. We found that opening windows and doors provided median ventilation of 28 air changes/hour (ACH), more than double that of mechanically ventilated negative-pressure rooms ventilated at the 12 ACH recommended for high-risk areas, and 18 times that with windows and doors closed (p < 0.001). Facilities built more than 50 years ago, characterised by large windows and high ceilings, had greater ventilation than modern naturally ventilated rooms (40 versus 17 ACH; p < 0.001). Even within the lowest quartile of wind speeds, natural ventilation exceeded mechanical (p < 0.001). The Wells-Riley airborne infection model predicted that in mechanically ventilated rooms 39% of susceptible individuals would become infected following 24 h of exposure to untreated TB patients of infectiousness characterised in a well-documented outbreak. This infection rate compared with 33% in modern and 11% in pre-1950 naturally ventilated facilities with windows and doors open.
Opening windows and doors maximises natural ventilation so that the risk of airborne contagion is much lower than with costly, maintenance-requiring mechanical ventilation systems. Old-fashioned clinical areas with high ceilings and large windows provide greatest protection. Natural ventilation costs little and is maintenance free, and is particularly suited to limited-resource settings and tropical climates, where the burden of TB and institutional TB transmission is highest. In settings where respiratory isolation is difficult and climate permits, windows and doors should be opened to reduce the risk of airborne contagion.
空气传播感染(如结核病)在医疗机构内的传播是一个重要的公共卫生问题,尤其是在资源有限的环境中,负压隔离病房等防护措施难以实施。自然通风可能提供一种低成本的替代方案。我们的目的是调查医疗机构中自然通风的速率、决定因素和效果。
该研究在秘鲁利马的八家医院进行;五家是1950年前建造的“老式”设计医院,三家是1970 - 1990年建造的“现代”设计医院。在这些医院中,研究了70间可能会遇到感染患者的自然通风临床病房。这些病房包括呼吸道隔离病房、结核病病房、呼吸内科病房、普通内科病房、门诊咨询室、候诊室和急诊科。将这些病房与2000年后建造的12间机械通风负压呼吸道隔离病房进行比较。在368次实验中使用二氧化碳示踪气体技术测量通风情况。测量建筑和环境变量。对于每次实验,使用空气传播感染的威尔斯 - 莱利模型估计结核病暴露的感染风险。我们发现,打开门窗时的平均通风量为每小时28次换气(ACH),是机械通风负压病房在高风险区域推荐的每小时12次换气量的两倍多,是门窗关闭时的18倍(p < 0.001)。50多年前建造的设施,其特点是窗户大、天花板高,通风效果比现代自然通风病房更好(分别为40次ACH和17次ACH;p < 0.001)。即使在风速最低的四分位数范围内,自然通风也超过机械通风(p < 0.001)。威尔斯 - 莱利空气传播感染模型预测,在机械通风病房中,易感个体在接触未治疗的具有在一次详细记录的疫情中所特征的传染性结核病患者24小时后,39%会被感染。与门窗打开时的现代自然通风设施中的33%以及1950年前自然通风设施中的11%的感染率相比。
打开门窗可使自然通风最大化,从而使空气传播传染的风险远低于昂贵且需要维护的机械通风系统。天花板高、窗户大的老式临床区域提供了最大的保护。自然通风成本低且无需维护,特别适合资源有限的环境和热带气候,在这些地方结核病负担和医疗机构内结核病传播负担最高。在呼吸道隔离困难且气候允许的环境中,应打开门窗以降低空气传播传染的风险。