Bell William C, Dallas Cham E
Center for Mass Destruction Defense, College of Pharmacy, University of Georgia, Athens, GA 30602, USA.
Int J Health Geogr. 2007 Feb 28;6:5. doi: 10.1186/1476-072X-6-5.
The threat posed by the use of weapons of mass destruction (WMD) within the United States has grown significantly in recent years, focusing attention on the medical and public health disaster capabilities of the nation in a large scale crisis. While the hundreds of thousands or millions of casualties resulting from a nuclear weapon would, in and of itself, overwhelm our current medical response capabilities, the response dilemma is further exacerbated in that these resources themselves would be significantly at risk. There are many limitations on the resources needed for mass casualty management, such as access to sufficient hospital beds including specialized beds for burn victims, respiration and supportive therapy, pharmaceutical intervention, and mass decontamination.
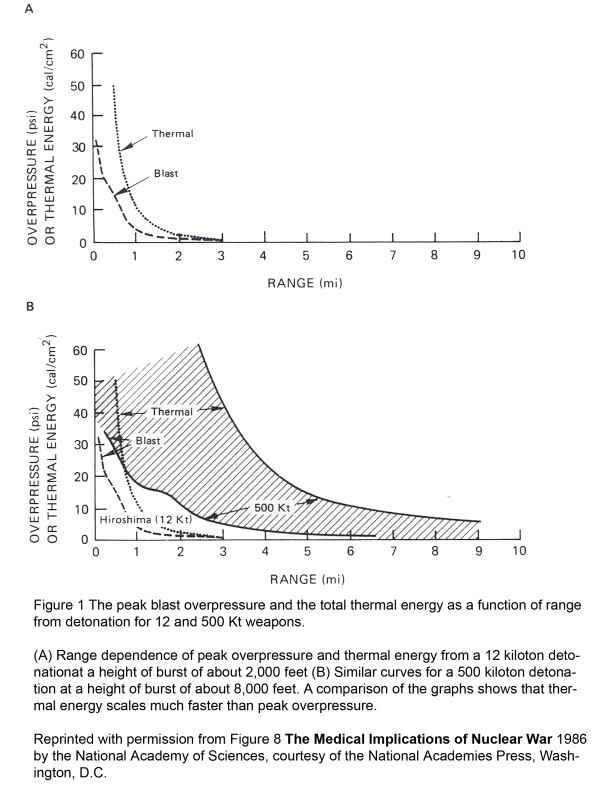
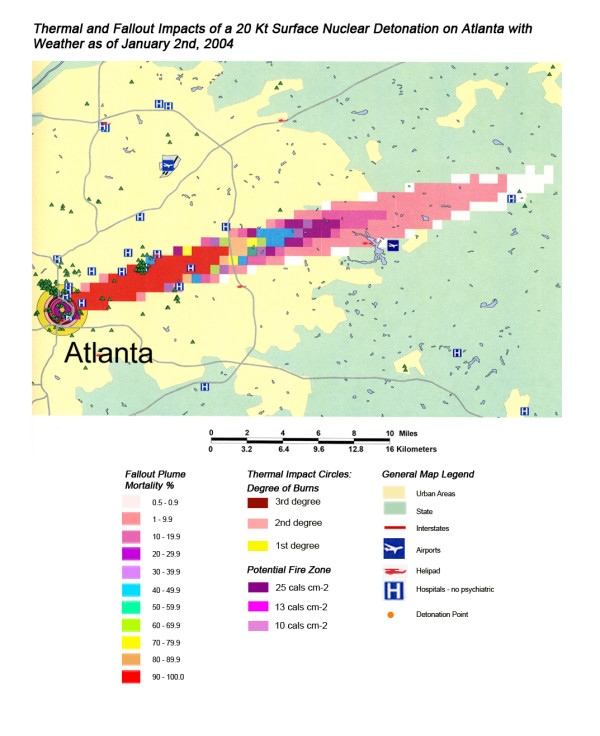
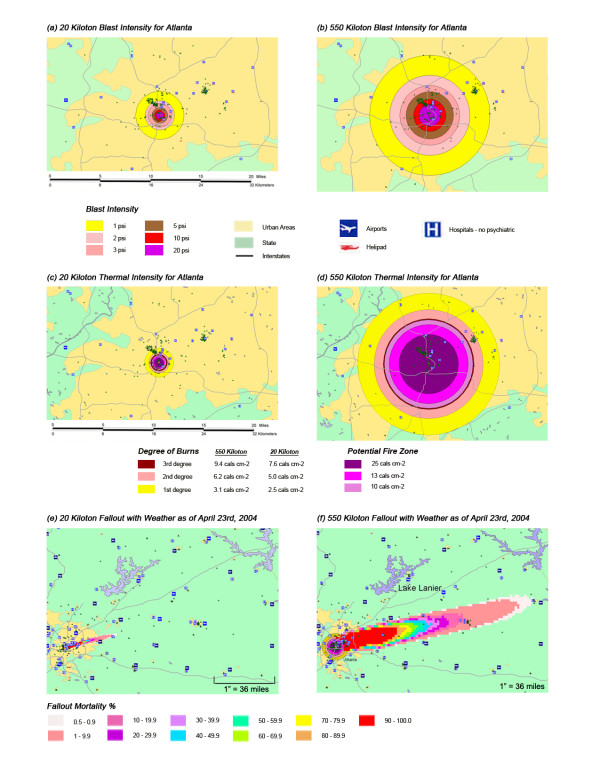
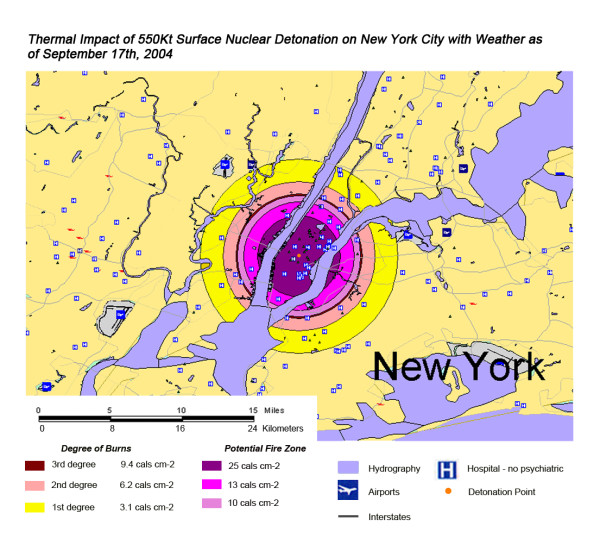
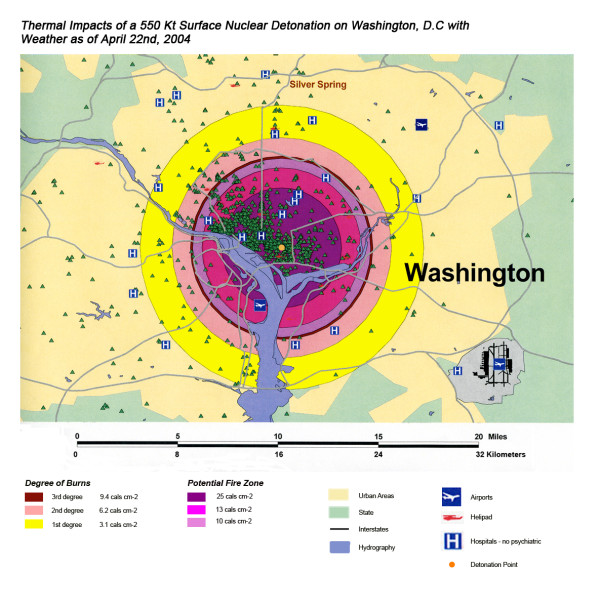
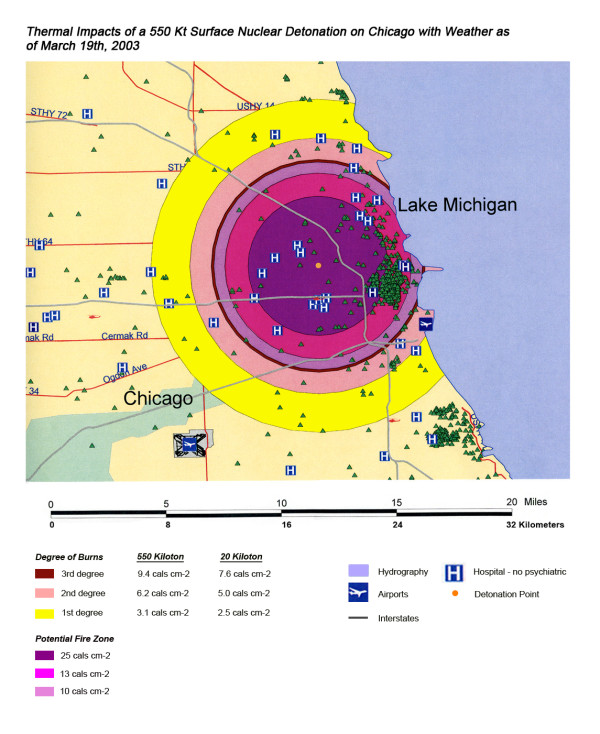
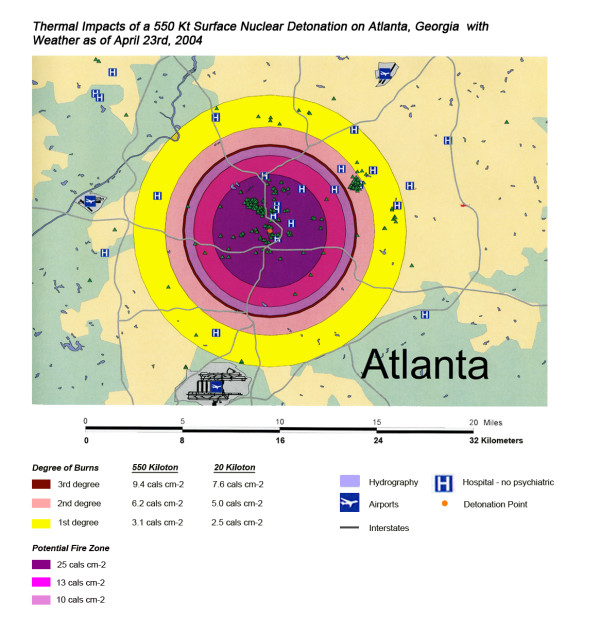
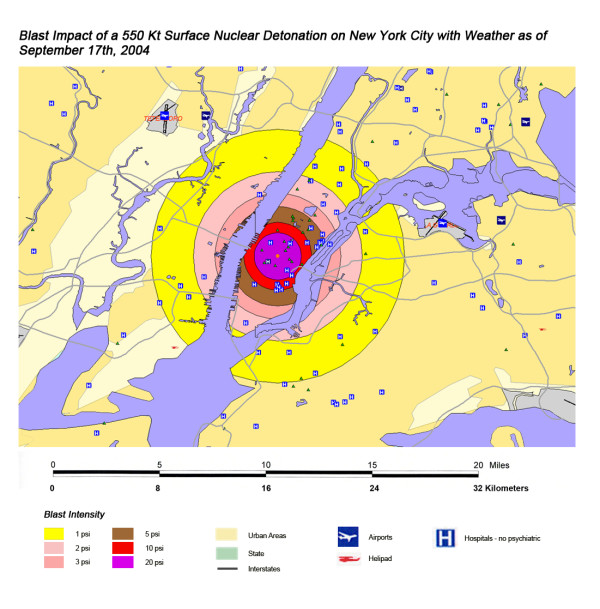
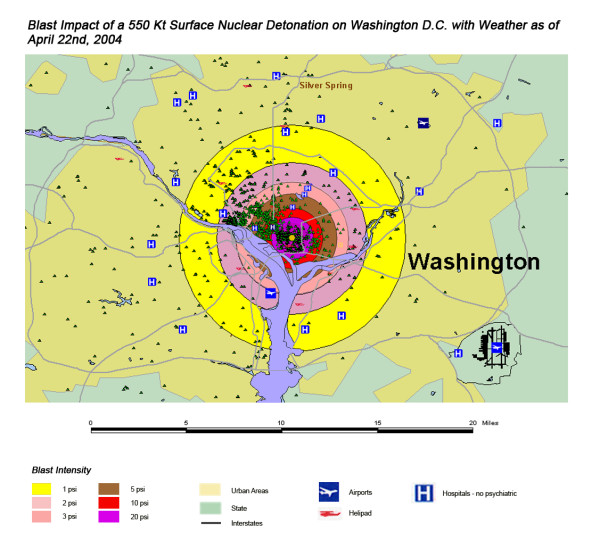
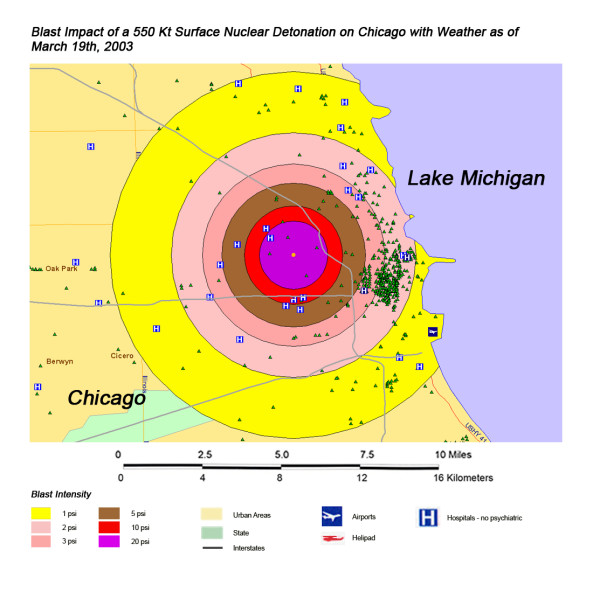
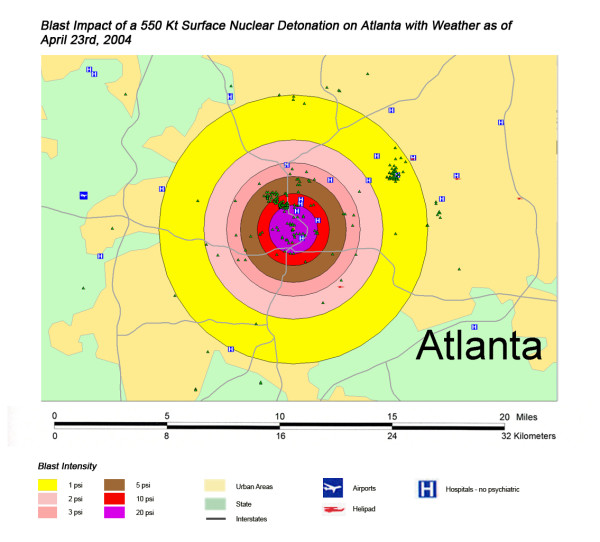
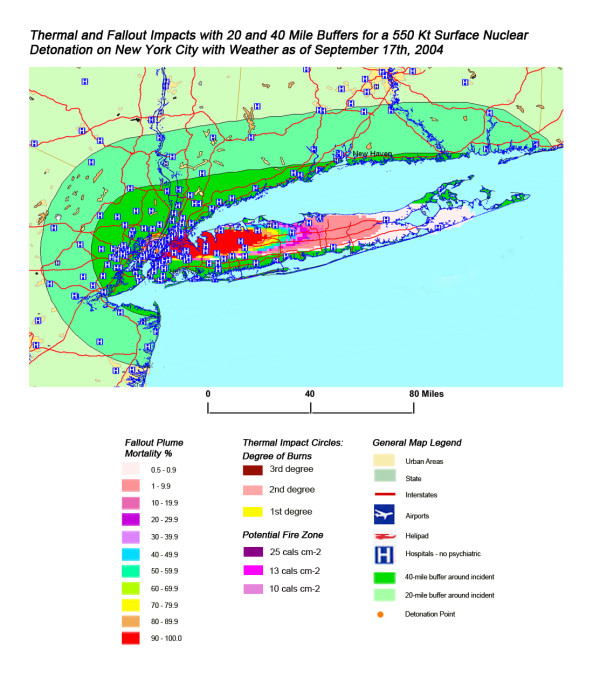
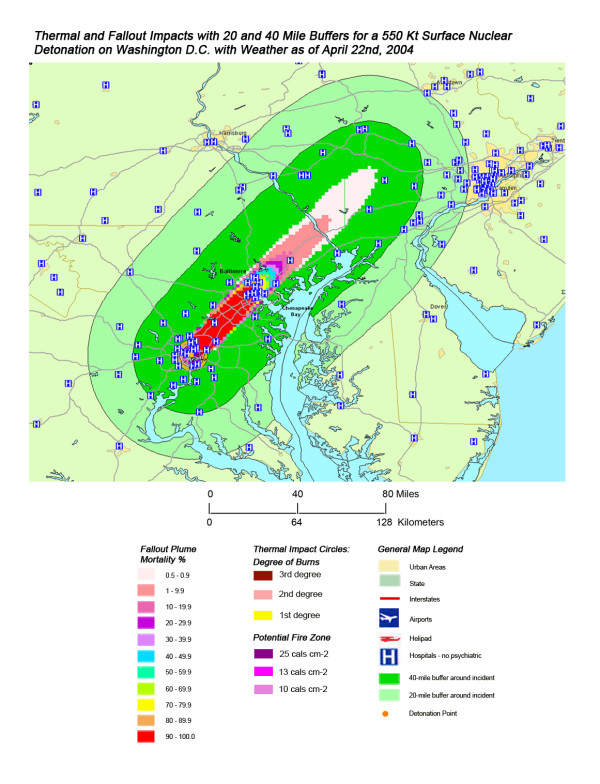
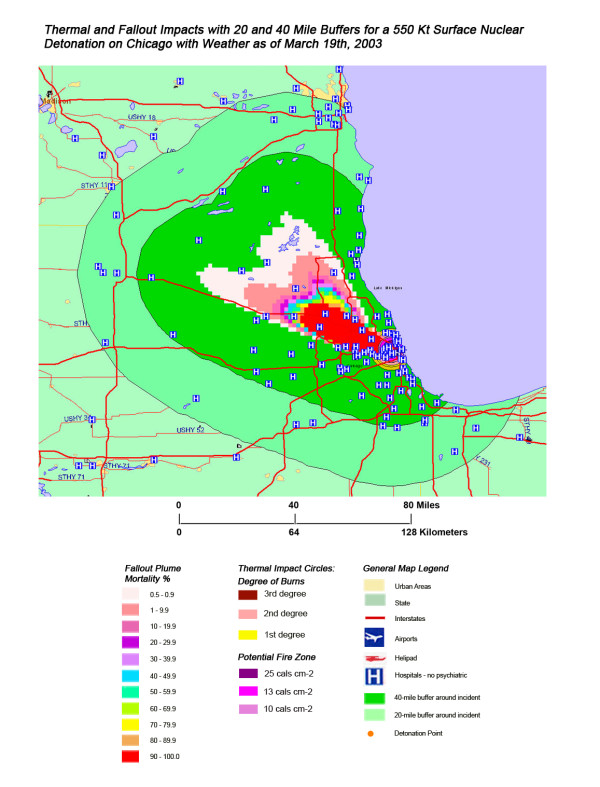
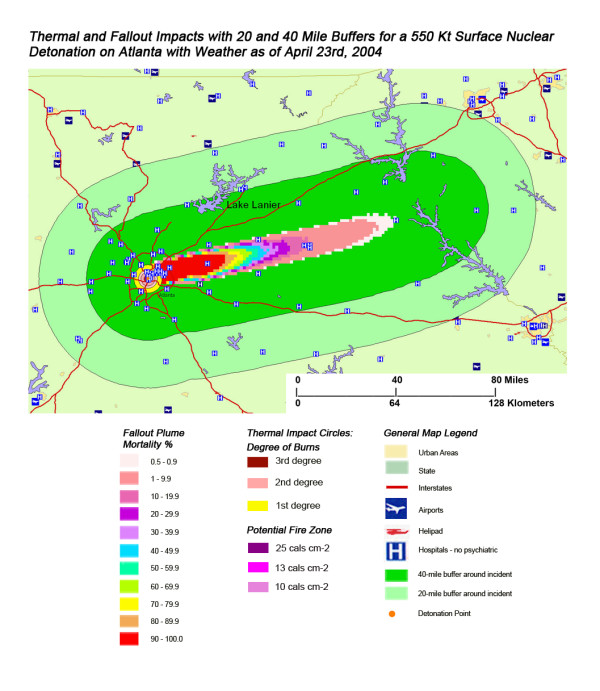
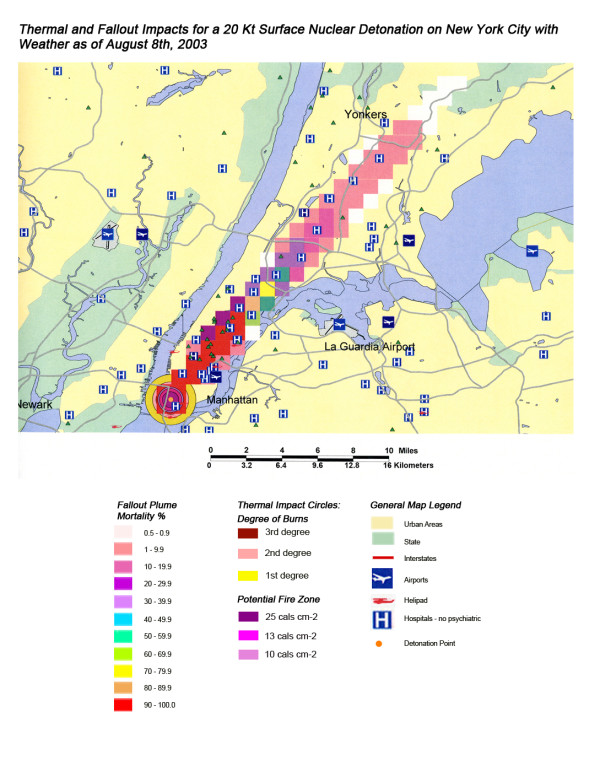
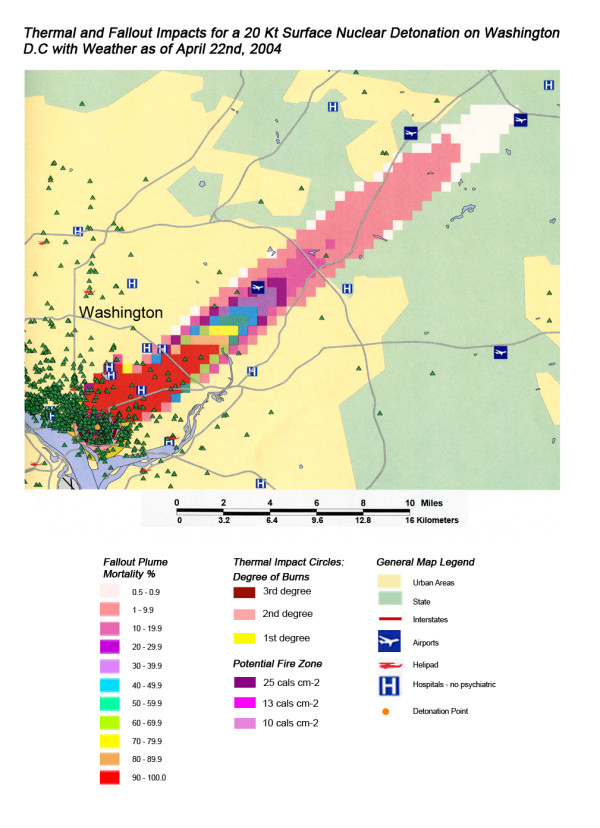
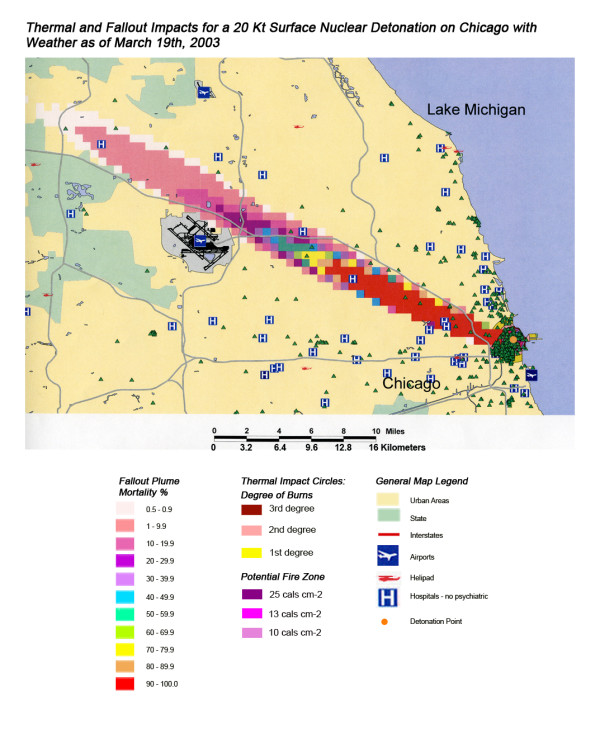
The effects of 20 kiloton and 550 kiloton nuclear detonations on high priority target cities are presented for New York City, Chicago, Washington D.C. and Atlanta. Thermal, blast and radiation effects are described, and affected populations are calculated using 2000 block level census data. Weapons of 100 Kts and up are primarily incendiary or radiation weapons, able to cause burns and start fires at distances greater than they can significantly damage buildings, and to poison populations through radiation injuries well downwind in the case of surface detonations. With weapons below 100 Kts, blast effects tend to be stronger than primary thermal effects from surface bursts. From the point of view of medical casualty treatment and administrative response, there is an ominous pattern where these fatalities and casualties geographically fall in relation to the location of hospital and administrative facilities. It is demonstrated that a staggering number of the main hospitals, trauma centers, and other medical assets are likely to be in the fatality plume, rendering them essentially inoperable in a crisis.
Among the consequences of this outcome would be the probable loss of command-and-control, mass casualties that will have to be treated in an unorganized response by hospitals on the periphery, as well as other expected chaotic outcomes from inadequate administration in a crisis. Vigorous, creative, and accelerated training and coordination among the federal agencies tasked for WMD response, military resources, academic institutions, and local responders will be critical for large-scale WMD events involving mass casualties.
近年来,在美国境内使用大规模杀伤性武器(WMD)所构成的威胁显著增加,这使得人们将注意力集中在国家在大规模危机中的医疗和公共卫生灾难应对能力上。虽然核武器造成的数十万或数百万人伤亡本身就会超出我们当前的医疗应对能力,但应对困境因这些资源自身也会面临巨大风险而进一步加剧。大规模伤亡管理所需资源存在诸多限制,例如获得足够的医院床位,包括为烧伤患者、呼吸及支持治疗设置的专用床位、药物干预以及大规模去污处理。
给出了2万吨级和55万吨级核爆炸对纽约市、芝加哥、华盛顿特区和亚特兰大等高优先级目标城市的影响。描述了热、冲击波和辐射效应,并使用2000年街区级人口普查数据计算了受影响人口。10万吨级及以上的武器主要是燃烧或辐射武器,在距离大于其对建筑物造成显著破坏的情况下,能够引发烧伤和火灾,并且在地面爆炸时,能通过下风向的辐射伤害毒害人群。对于低于10万吨级的武器,地面爆炸产生的冲击波效应往往比主要热效应更强。从医疗伤亡救治和行政应对的角度来看,存在一种不祥的模式,即这些死亡和伤亡在地理上与医院和行政设施的位置相关。结果表明,大量主要医院、创伤中心及其他医疗资源可能处于死亡羽流中,这使得它们在危机中基本无法运作。
这一结果的后果包括可能失去指挥与控制、大量伤亡人员将不得不由周边医院在无组织的应对中进行救治,以及危机中行政管理不足引发的其他预期混乱局面。对于涉及大量伤亡的大规模WMD事件,由负责WMD应对的联邦机构、军事资源、学术机构和地方应对人员之间进行积极、创新和加速的培训与协调至关重要。