Corbeel Lucien
Department of Pediatrics, University Hospital, Herestraat 49, Leuven, Belgium.
Eur J Pediatr. 2007 Jun;166(6):511-9. doi: 10.1007/s00431-007-0461-8. Epub 2007 Mar 16.
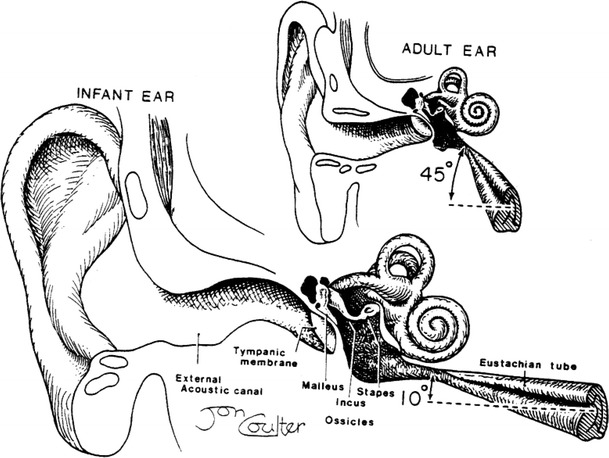
The "wait and see" approach in acute otitis media (AOM), consisting of postponing the antibiotic administration for a few days, has been advocated mainly to counteract the increased bacterial resistance in respiratory infections. This approach is not justified in children less than 2 years of age and this for several reasons. First, AOM is an acute inflammation of the middle ear caused in about 70% of cases by bacteria. Redness and bulging of the tympanic membrane are characteristic findings in bacterial AOM. Second, AOM is associated with long-term dysfunction of the inflamed eustachian tube (ET), particularly in children less than 2 years of age. In this age group, the small calibre of the ET together with its horizontal direction result in impaired clearance, ventilation and protection of the middle ear. Third, recent prospective studies have shown poor long-term prognosis of AOM in children below 2 years with at least 50% of recurrences and persisting otitis media with effusion (OME) in about 35% 6 months after AOM. Viruses elicit AOM in about 30% of children. A prolonged course of AOM has been observed when bacterial and viral infections are combined because viral infection is also associated with ET dysfunction in young children. Bacterial and viral testing of the nasopharyngeal aspirate is an excellent tool both for initial treatment and recurrence of AOM. Antibiotic treatment of AOM is mandatory in children less than 2 years of age to decrease inflammation in the middle ear but also of the ET particularly during the first episode. The best choice is amoxicillin because of its superior penetration in the middle ear. Streptococci pneumoniae with intermediary bacterial resistance to penicillin are particularly associated with recurrent AOM. Therefore the dosage of amoxicillin should be 90 mg/kg per day in three doses. In recurrent AOM with beta-lactamase-producing bacilli, amoxicillin should be associated with clavulanic acid at a dose of 6.4 mg/kg per day. The duration of the treatment is not established yet but 10 days is reasonable for a first episode of AOM. OME may be a precursor initiating AOM but also a complication thereof. OME needs a watchful waiting approach. When associated with deafness for 2-3 months in children over 2 years of age, an antibiotic should be given according to the results of the bacterial resistance in the nasopharyngeal aspirate. The high rate of complications of tympanostomy tube insertion outweighs the beneficial effect on hearing loss. The poor results of this procedure are due to the absence of effects on ET dysfunction. Pneumococcal vaccination has little beneficial effects on recurrent AOM and its use in infants needs further studies. Treatment with amoxicillin is indicated in all children younger than 2 years with a first episode of AOM presenting with redness and bulging of the tympanic membrane. Combined amoxicillin and clavulanic acid should be given in patients with beta-lactamase-producing bacteria. The duration of treatment is estimated to be at least 10 days depending on the findings by pneumo-otoscopy and tympanometry. Bacterial and viral testing of the nasopharyngeal aspirate is highly recommended particularly in children in day care centres as well as for regular follow-up. The high recurrence rate is due to the long-lasting dysfunction of the eustachian tube and the immune immaturity of children less than 2 years of age.
急性中耳炎(AOM)的“观察等待”方法,即推迟数天使用抗生素,主要是为了应对呼吸道感染中细菌耐药性增加的问题。这种方法对2岁以下儿童并不适用,原因有以下几点。首先,AOM是中耳的急性炎症,约70%的病例由细菌引起。鼓膜发红和膨出是细菌性AOM的特征性表现。其次,AOM与发炎的咽鼓管(ET)长期功能障碍有关,尤其是在2岁以下儿童中。在这个年龄组中,ET管径小且走向水平,导致中耳的清除、通气和保护功能受损。第三,最近的前瞻性研究表明,2岁以下儿童AOM的长期预后较差,至少50%会复发,约35%在AOM后6个月会持续存在中耳积液(OME)。约30%的儿童AOM由病毒引起。当细菌和病毒感染合并时,会观察到AOM病程延长,因为病毒感染也与幼儿的ET功能障碍有关。鼻咽抽吸物的细菌和病毒检测是AOM初始治疗和复发治疗的优秀工具。2岁以下儿童AOM必须使用抗生素治疗,以减轻中耳炎症,尤其是ET的炎症,特别是在首次发作时。最佳选择是阿莫西林,因为它在中耳的穿透力更强。对青霉素具有中度细菌耐药性的肺炎链球菌与复发性AOM特别相关。因此,阿莫西林的剂量应为每天90mg/kg,分三次服用。对于产β-内酰胺酶杆菌引起的复发性AOM,阿莫西林应与克拉维酸联合使用,剂量为每天6.4mg/kg。治疗持续时间尚未确定,但AOM首次发作时10天是合理的。OME可能是引发AOM的先兆,也是其并发症。OME需要密切观察等待。当2岁以上儿童OME伴有2 - 3个月的听力丧失时,应根据鼻咽抽吸物细菌耐药性检测结果给予抗生素治疗。鼓膜置管术的高并发症发生率超过了其对听力损失的有益效果。该手术效果不佳是因为对ET功能障碍没有作用。肺炎球菌疫苗对复发性AOM几乎没有有益效果,其在婴儿中的使用需要进一步研究。所有2岁以下首次发作AOM且鼓膜发红和膨出的儿童均应使用阿莫西林治疗。对于产β-内酰胺酶细菌的患者,应给予阿莫西林和克拉维酸联合治疗。根据耳镜检查和鼓室图检查结果,治疗持续时间估计至少为10天。强烈建议对鼻咽抽吸物进行细菌和病毒检测,尤其是在日托中心的儿童以及定期随访时。高复发率是由于咽鼓管长期功能障碍以及2岁以下儿童免疫不成熟所致。