Heringlake Matthias, Wernerus Marit, Grünefeld Julia, Klaus Stephan, Heinze Hermann, Bechtel Matthias, Bahlmann Ludger, Poeling Jochen, Schön Julika
Department of Anesthesiology, Universität zu Lübeck, D-23538 Lübeck, Germany.
Crit Care. 2007;11(2):R51. doi: 10.1186/cc5904.
Myocardial dysfunction necessitating inotropic support is a typical complication after on-pump cardiac surgery. This prospective, randomized pilot study analyzes the metabolic and renal effects of the inotropes adrenaline and milrinone in patients needing inotropic support after coronary artery bypass grafting (CABG).
During an 18-month period, 251 patients were screened for low cardiac output upon intensive care unit (ICU) admission after elective, isolated CABG surgery. Patients presenting with a cardiac index (CI) of less than 2.2 liters/minute per square meter upon ICU admission - despite adequate mean arterial (titrated with noradrenaline or sodium nitroprusside) and filling pressures - were randomly assigned to 14-hour treatment with adrenaline (n = 7) or milrinone (n = 11) to achieve a CI of greater than 3.0 liters/minute per square meter. Twenty patients not needing inotropes served as controls. Hemodynamics, plasma lactate, pyruvate, glucose, acid-base status, insulin requirements, the urinary excretion of alpha-1-microglobuline, and creatinine clearance were determined during the treatment period, and cystatin-C levels were determined up to 48 hours after surgery (follow-up period).
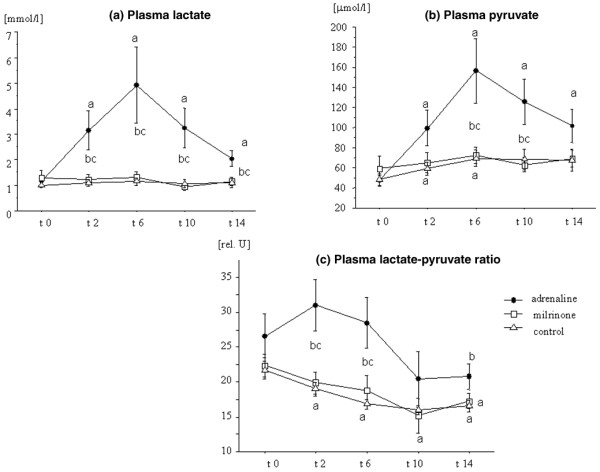
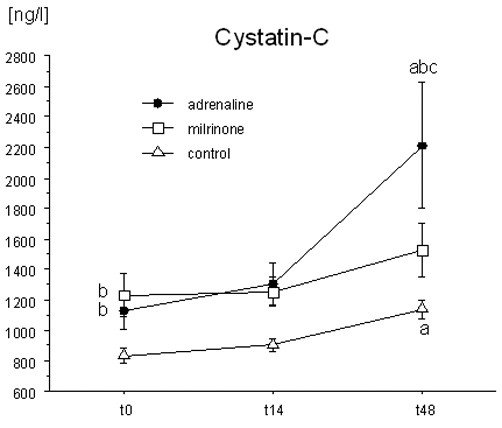
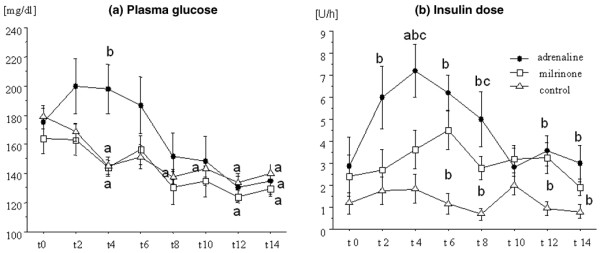
After two to four hours after ICU admission, the target CI was achieved in both intervention groups and maintained during the observation period. Plasma lactate, pyruvate, the lactate/pyruvate ratio, plasma glucose, and insulin doses were higher (p < 0.05) in the adrenaline-treated patients than during milrinone or control conditions. The urinary excretion of alpha-1-microglobuline was higher in the adrenaline than in the control group 6 to 14 hours after admission (p < 0.05). No between-group differences were observed in creatinine clearance, whereas plasma cystatin-C levels were significantly higher in the adrenaline than in the milrinone or the control group after 48 hours (p < 0.05).
This suggests that the use of adrenaline for the treatment of postoperative myocardial dysfunction - in contrast to treatment with the PDE-III inhibitor milrinone - is associated with unwarranted metabolic and renal effects.
需要使用正性肌力药物支持的心肌功能障碍是心脏搭桥手术后的典型并发症。这项前瞻性、随机对照试验研究分析了肾上腺素和米力农这两种正性肌力药物对冠状动脉搭桥术(CABG)后需要正性肌力药物支持的患者的代谢和肾脏影响。
在18个月的时间里,对251例择期、单纯CABG手术后入住重症监护病房(ICU)的患者进行了低心输出量筛查。尽管平均动脉压(用去甲肾上腺素或硝普钠滴定)和充盈压正常,但入住ICU时心脏指数(CI)低于2.2升/分钟/平方米的患者被随机分配接受14小时的肾上腺素(n = 7)或米力农(n = 11)治疗,以使CI大于3.0升/分钟/平方米。20例不需要正性肌力药物的患者作为对照。在治疗期间测定血流动力学、血浆乳酸、丙酮酸、葡萄糖、酸碱状态、胰岛素需求量、α-1-微球蛋白尿排泄量和肌酐清除率,并在术后48小时(随访期)测定胱抑素-C水平。
入住ICU后两到四小时,两个干预组均达到目标CI,并在观察期内维持。肾上腺素治疗组患者的血浆乳酸、丙酮酸、乳酸/丙酮酸比值、血浆葡萄糖和胰岛素剂量高于米力农治疗组或对照组(p < 0.05)。入住后6至14小时,肾上腺素组的α-1-微球蛋白尿排泄量高于对照组(p < 0.05)。肌酐清除率在组间无差异,而术后48小时肾上腺素组的血浆胱抑素-C水平显著高于米力农组或对照组(p < 0.05)。
这表明,与使用磷酸二酯酶III抑制剂米力农治疗相比,使用肾上腺素治疗术后心肌功能障碍会产生不必要的代谢和肾脏影响。