Ho Vivian, Petersen Laura A
Baker Institute, Rice University, 6100 Main Street, Houston, TX 77005, USA.
Cost Eff Resour Alloc. 2007 Jun 29;5:7. doi: 10.1186/1478-7547-5-7.
We examined whether higher procedure volumes for coronary artery bypass graft (CABG) surgery or percutaneous coronary interventions (PCI) were associated with lower costs per patient, and if so, estimated the financial savings from regionalizing cardiac procedures.
Cost regressions with hospital-specific dummy variables measured within-hospital cost reductions associated with increasing hospital volume. We used the regression estimates to predict the change in total costs that would result from moving patients in low-volume hospitals to higher volume facilities.
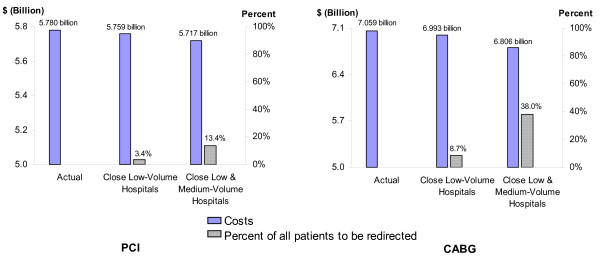
A 10% increase in PCI procedure volume lowered costs per patient by 0.7%. For the average hospital performing CABG in 2000, a 10% increase in volume was associated with a 2.8% reduction in average costs. Despite these lower costs, the predicted savings from regionalizing all PCI procedures in the sample from lower to high-volume hospitals amounted to only 1.1% of the entire costs of performing PCI procedures for the sample in 2000. Similarly, the cost savings for CABG were estimated to be only 3.5%.
Higher volumes were associated with lower costs per procedure. However, the total potential savings from regionalizing cardiac procedures is relatively minor, and may not justify the risks of reducing access to needed services.
我们研究了冠状动脉搭桥术(CABG)或经皮冠状动脉介入治疗(PCI)的手术量增加是否与每位患者的成本降低相关,如果是这样,则估计了将心脏手术区域化带来的财务节省。
采用带有医院特定虚拟变量的成本回归来衡量与医院手术量增加相关的院内成本降低情况。我们使用回归估计来预测将低手术量医院的患者转移到高手术量医院所导致的总成本变化。
PCI手术量增加10%可使每位患者的成本降低0.7%。对于2000年进行CABG的平均医院而言,手术量增加10%与平均成本降低2.8%相关。尽管成本降低了,但将样本中所有PCI手术从低手术量医院转移到高手术量医院所预测的节省仅占2000年样本中PCI手术总成本的1.1%。同样,CABG的成本节省估计仅为3.5%。
手术量增加与每个手术的成本降低相关。然而,将心脏手术区域化带来的潜在总节省相对较小,可能不足以证明减少获得所需服务的风险是合理的。