Department of Radiation Oncology, The University of Texas Health Science Center at San Antonio, San Antonio, TX, USA.
Radiat Oncol. 2007 Jul 14;2:26. doi: 10.1186/1748-717X-2-26.
Intensity-modulated radiation therapy (IMRT) affords unparalleled capacity to deliver conformal radiation doses to tumors in the central nervous system. However, to date, there are few reported outcomes from using IMRT, either alone or as a boost technique, for standard fractionation radiotherapy for glioblastoma multiforme (GBM).
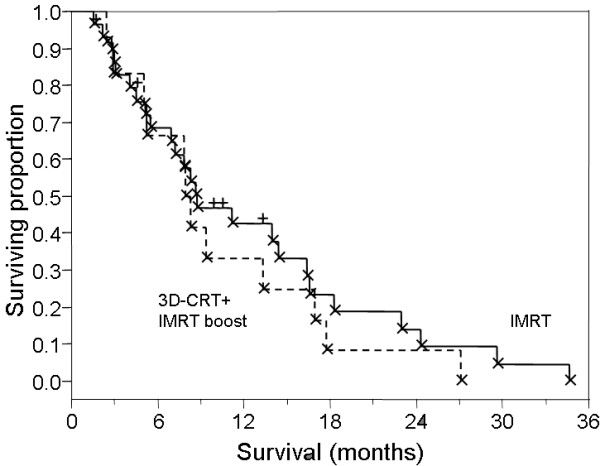
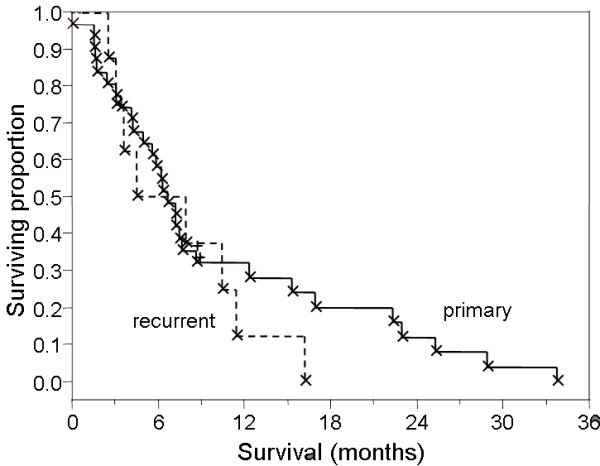
Forty-two patients were treated with IMRT alone (72%) or as a boost (28%) after 3-dimensional conformal radiation therapy (3D-CRT). Thirty-three patients with primary disease and 9 patients with recurrent tumors were included. Thirty-four patients (81%) had surgery, with gross tumor resection in 13 patients (36%); 22 patients (53%) received chemo-radiotherapy. The median total radiation dose for all patients was 60 Gy with a range from 30.6 to 74 Gy. Standard fractions of 1.8 Gy/day to 2.0 Gy/day were utilized.
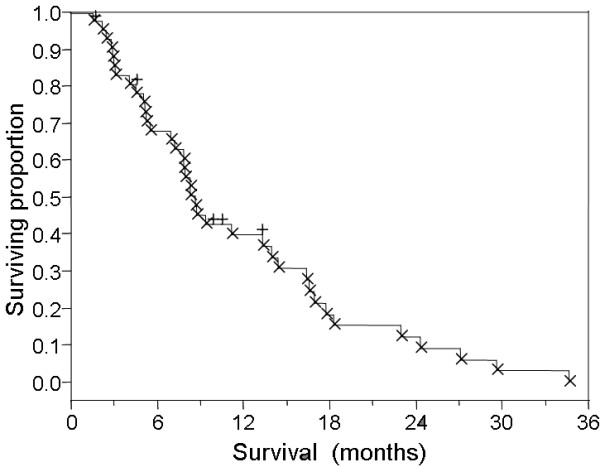
Median survival was 8.7 months, with 37 patients (88%) deceased at last contact. Nonparametric analysis showed no survival difference in IMRT-boost vs. IMRT-only groups.
While technically feasible, preliminary results suggest delivering standard radiation doses by IMRT did not improve survival outcomes in this series compared to historical controls. In light of this lack of a survival benefit and the costs associated with use of IMRT, future prospective trials are needed to evaluate non-survival endpoints such as quality of life and functional preservation. Short of such evidence, the use of IMRT for treatment of GBM needs to be carefully rationalized.
调强放射治疗(IMRT)为中枢神经系统肿瘤提供了无与伦比的适形放射剂量能力。然而,迄今为止,单独使用 IMRT 或作为推量技术,用于多形性胶质母细胞瘤(GBM)的标准分割放疗,其结果鲜有报道。
42 例患者单独接受 IMRT(72%)或 3 维适形放射治疗(3D-CRT)后接受 IMRT 推量(28%)治疗。包括原发性疾病 33 例和复发性肿瘤 9 例。34 例患者(81%)接受了手术,其中 13 例(36%)行大体肿瘤切除术;22 例(53%)接受了放化疗。所有患者的中位总放射剂量为 60Gy,范围为 30.6 至 74Gy。标准分割剂量为 1.8Gy/天至 2.0Gy/天。
中位生存期为 8.7 个月,最后随访时 37 例患者(88%)死亡。非参数分析显示,IMRT 推量组与 IMRT 单纯组之间的生存无差异。
虽然技术上可行,但初步结果表明,与历史对照相比,在本系列中,IMRT 标准剂量治疗并未改善生存结果。鉴于没有生存获益,以及使用 IMRT 相关的成本,需要进行前瞻性试验来评估非生存终点,如生活质量和功能保留。在缺乏这种证据的情况下,需要谨慎地合理化使用 IMRT 治疗 GBM。