van de Poll Marcel C G, Derikx Joep P M, Buurman Wim A, Peters Wilbert H M, Roelofs Hennie M J, Wigmore Stephen J, Dejong Cornelis Hc
Department of Surgery, University Hospital Maastricht and Nutrition and Toxicology Research Institute (NUTRIM), Maastricht University, Maastricht, The Netherlands.
World J Surg. 2007 Oct;31(10):2033-8. doi: 10.1007/s00268-007-9182-4.
Liver failure following liver surgery is caused by an insufficient functioning remnant cell mass. This can be due to insufficient liver volume and can be aggravated by additional cell death during or after surgery. The aim of this study was to elucidate the causes of hepatocellular injury in patients undergoing liver resection.
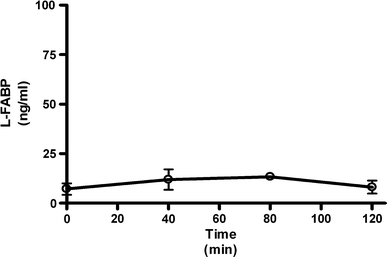
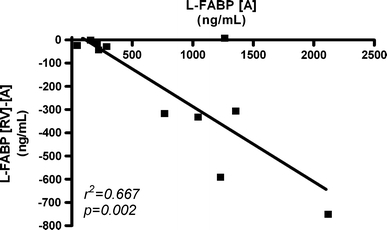
Markers of hepatocyte injury (AST, GSTalpha, and L-FABP) and inflammation (IL-6) were measured in plasma of patients undergoing liver resection with and without intermittent inflow occlusion. To study the separate involvement of the intestines and the liver in systemic L-FABP release, arteriovenous concentration differences for L-FABP were measured.
During liver manipulation, liver injury markers increased significantly. Arterial plasma levels and transhepatic and transintestinal concentration gradients of L-FABP indicated that this increase was exclusively due to hepatic and not due to intestinal release. Intermittent hepatic inflow occlusion, anesthesia, and liver transection did not further enhance arterial L-FABP and GSTalpha levels. Hepatocyte injury was followed by an inflammatory response.
This study shows that liver manipulation is a leading cause of hepatocyte injury during liver surgery. A potential causal relation between liver manipulation and systemic inflammation remains to be established; but since the inflammatory response is apparently initiated early during major abdominal surgery, interventions aimed at reducing postoperative inflammation and related complications should be started early during surgery or beforehand.
肝脏手术后的肝衰竭是由残余肝细胞团功能不足引起的。这可能是由于肝脏体积不足,并且在手术期间或手术后额外的细胞死亡会使其加重。本研究的目的是阐明肝切除患者肝细胞损伤的原因。
在有或无间歇性入肝血流阻断的肝切除患者血浆中测量肝细胞损伤标志物(AST、GSTα和L-FABP)和炎症标志物(IL-6)。为了研究肠道和肝脏在全身L-FABP释放中的单独作用,测量了L-FABP的动静脉浓度差。
在肝脏手术操作期间,肝脏损伤标志物显著增加。L-FABP的动脉血浆水平以及经肝和经肠浓度梯度表明,这种增加完全是由于肝脏释放而非肠道释放。间歇性肝血流阻断、麻醉和肝横断并未进一步提高动脉L-FABP和GSTα水平。肝细胞损伤后会出现炎症反应。
本研究表明,肝脏手术操作是肝手术期间肝细胞损伤的主要原因。肝脏手术操作与全身炎症之间的潜在因果关系仍有待确立;但由于炎症反应显然在大型腹部手术早期就已启动,旨在减少术后炎症及相关并发症的干预措施应在手术早期或术前开始实施。