Jeschke Marc G, Mlcak Ronald P, Finnerty Celeste C, Norbury William B, Gauglitz Gerd G, Kulp Gabriela A, Herndon David N
Shriners Hospitals for Children, 815 Market Street, Galveston, TX 77550, USA.
Crit Care. 2007;11(4):R90. doi: 10.1186/cc6102.
Increased burn size leads to increased mortality of burned patients. Whether mortality is due to inflammation, hypermetabolism or other pathophysiologic contributing factors is not entirely determined. The purpose of the present study was to determine in a large prospective clinical trial whether different burn sizes are associated with differences in inflammation, body composition, protein synthesis, or organ function.
Pediatric burned patients were divided into four burn size groups: <40% total body surface area (TBSA) burn, 40-59% TBSA burn, 60-79% TBSA burn, and >80% TBSA burn. Demographic and clinical data, hypermetabolism, the inflammatory response, body composition, the muscle protein net balance, serum and urine hormones and proteins, and cardiac function and changes in liver size were determined.
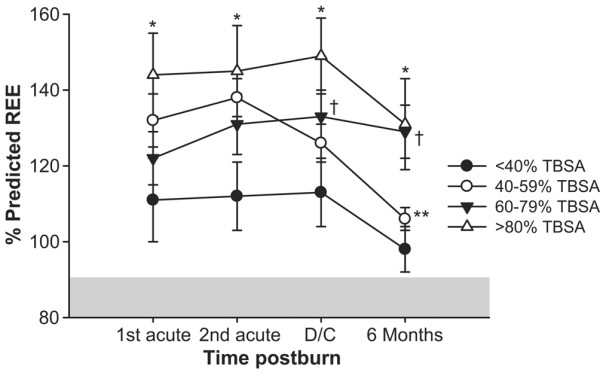
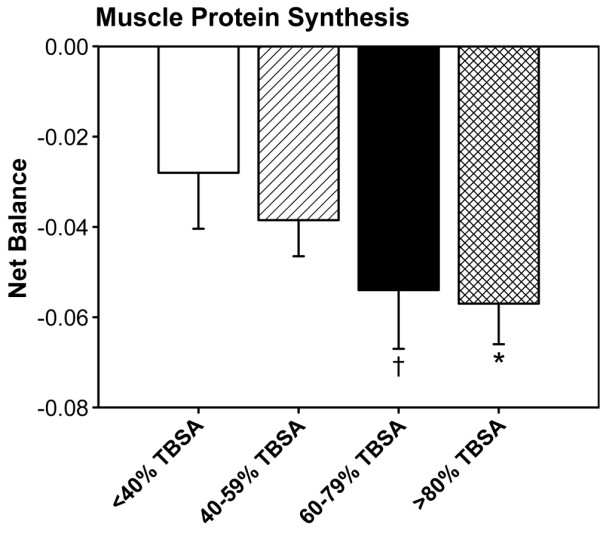
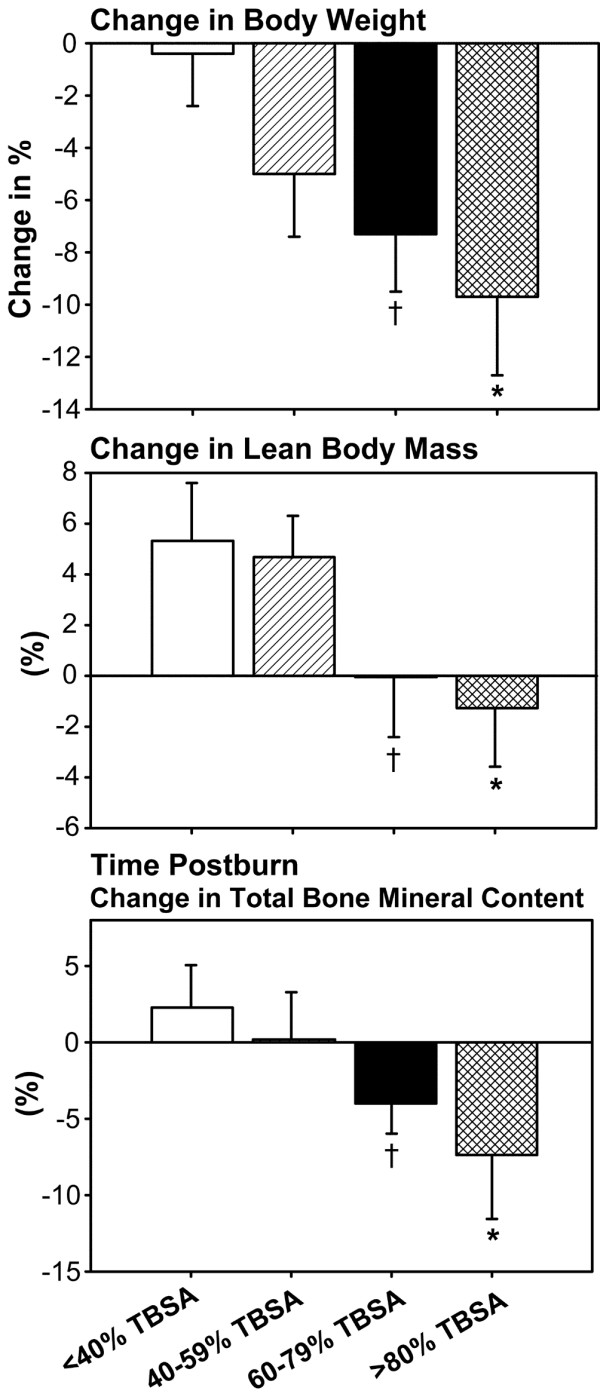
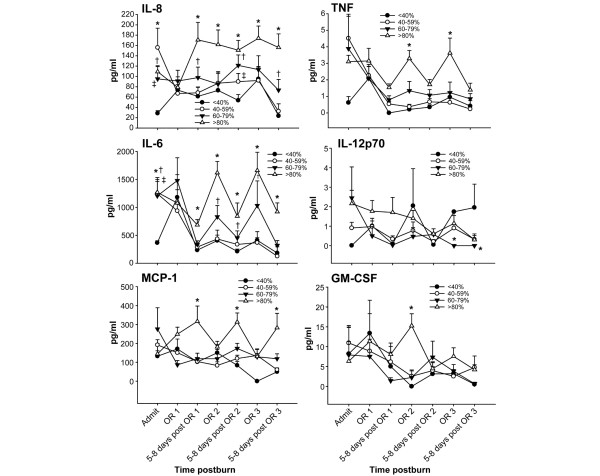
One hundred and eighty-nine pediatric patients of similar age and gender distribution were included in the study (<40% TBSA burn, n = 43; 40-59% TBSA burn, n = 79; 60-79% TBSA burn, n = 46; >80% TBSA burn, n = 21). Patients with larger burns had more operations, a greater incidence of infections and sepsis, and higher mortality rates compared with the other groups (P < 0.05). The percentage predicted resting energy expenditure was highest in the >80% TBSA group, followed by the 60-79% TBSA burn group (P < 0.05). Children with >80% burns lost the most body weight, lean body mass, muscle protein and bone mineral content (P < 0.05). The urine cortisol concentration was highest in the 80-99% and 60-79% TBSA burn groups, associated with significant myocardial depression and increased change in liver size (P < 0.05). The cytokine profile showed distinct differences in expression of IL-8, TNF, IL-6, IL-12p70, monocyte chemoattractant protein-1 and granulocyte-macrophage colony-stimulating factor (P < 0.05).
Morbidity and mortality in burned patients is burn size dependent, starts at a 60% TBSA burn and is due to an increased hypermetabolic and inflammatory reaction, along with impaired cardiac function.
烧伤面积增加会导致烧伤患者死亡率上升。死亡率是由炎症、高代谢还是其他病理生理因素所致尚未完全明确。本研究的目的是在一项大型前瞻性临床试验中确定不同烧伤面积是否与炎症、身体成分、蛋白质合成或器官功能的差异相关。
将小儿烧伤患者分为四个烧伤面积组:全身表面积(TBSA)烧伤<40%、40 - 59% TBSA烧伤、60 - 79% TBSA烧伤和>80% TBSA烧伤。测定人口统计学和临床数据、高代谢、炎症反应、身体成分、肌肉蛋白净平衡、血清和尿液中的激素及蛋白质,以及心脏功能和肝脏大小变化。
189名年龄和性别分布相似的小儿患者纳入研究(<40% TBSA烧伤,n = 43;40 - 59% TBSA烧伤,n = 79;60 - 79% TBSA烧伤,n = 46;>80% TBSA烧伤,n = 21)。与其他组相比,烧伤面积较大的患者手术更多、感染和脓毒症发生率更高、死亡率更高(P < 0.05)。预计静息能量消耗百分比在>80% TBSA组最高,其次是60 - 79% TBSA烧伤组(P < 0.05)。烧伤面积>80%的儿童体重、瘦体重、肌肉蛋白和骨矿物质含量损失最多(P < 0.05)。80 - 99%和60 - 79% TBSA烧伤组尿液皮质醇浓度最高,伴有明显的心肌抑制和肝脏大小变化增加(P < 0.05)。细胞因子谱显示白细胞介素-8、肿瘤坏死因子、白细胞介素-6、白细胞介素-12p70、单核细胞趋化蛋白-1和粒细胞-巨噬细胞集落刺激因子的表达存在明显差异(P < 0.05)。
烧伤患者的发病率和死亡率取决于烧伤面积,从60% TBSA烧伤开始,是由于高代谢和炎症反应增加以及心脏功能受损所致。