Keus Frederik, de Vries Jolanda, Gooszen Hein G, van Laarhoven Cornelis J H M
Department of Surgery, Diakonessenhuis, Bosboomstraat 1, 3582, KE, Utrecht, The Netherlands.
Surg Endosc. 2008 Jul;22(7):1649-59. doi: 10.1007/s00464-007-9675-0. Epub 2007 Dec 11.
Gallstones are a major cause of morbidity, and cholecystectomy is a commonly performed procedure. Minimal invasive procedures, laparoscopic cholecystectomy (LC) and small-incision cholecystectomy (SIC), have replaced the classical open cholecystectomy. No differences have been found in primary outcome measures between LC and SIC, therefore secondary outcome measures have to be considered to determine preferences. The aim of our study was to examine health status applying evidence-based guidelines in LC and SIC in a randomised trial.
Patients with symptomatic cholecystolithiasis were included in a blind randomised trial. Operative procedures, anaesthesia, analgesics and postoperative care were standardised in order to limit bias. Questionnaires were filled in preoperatively, the first day postoperatively, and at outpatients follow-up at 2, 6 and 12 weeks. In accordance with evidence-based guidelines, the generic short form (SF-36) and the disease-specific gastrointestinal quality-of-life index (GIQLI) questionnaires were used in addition to the body image questionnaire (BIQ).
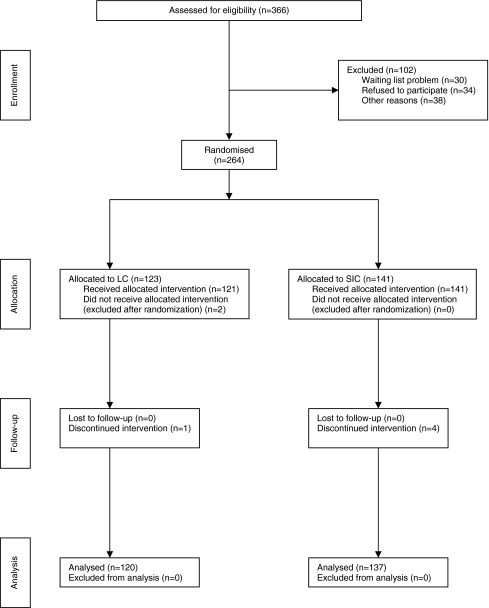
A total of 257 patients were randomised between LC (120) and SIC (137). Analyses were performed according to intention-to-treat (converted procedures included) and also distinguishing converted from minimal invasive (nonconverted) procedures. Questionnaires were obtained with a response rate varying from 87.5% preoperatively to 77.4% three months postoperatively. Except for two time-specific measurements in one SF-36 subscale, there were no differences between LC and SIC. There were significant differences in several subscales in all three questionnaires comparing minimal invasive versus converted procedures.
Applying adequate methodological quality and evidence-based guidelines (by using SF-36 and GIQLI), there are no significant differences in health status between LC and SIC.
胆结石是发病的主要原因,胆囊切除术是一种常见的手术。微创手术,即腹腔镜胆囊切除术(LC)和小切口胆囊切除术(SIC),已取代了传统的开腹胆囊切除术。在LC和SIC的主要结局指标上未发现差异,因此必须考虑次要结局指标以确定偏好。我们研究的目的是在一项随机试验中,应用循证指南检查LC和SIC患者的健康状况。
有症状的胆囊结石患者被纳入一项双盲随机试验。为了限制偏倚,对手术操作、麻醉、镇痛和术后护理进行了标准化。术前、术后第一天以及术后2周、6周和12周门诊随访时填写问卷。根据循证指南,除了身体形象问卷(BIQ)外,还使用了通用简表(SF-36)和疾病特异性胃肠道生活质量指数(GIQLI)问卷。
共有257例患者被随机分为LC组(120例)和SIC组(137例)。分析按照意向性分析进行(包括中转手术),并区分中转手术和微创手术(未中转手术)。问卷的回收率从术前的87.5%到术后3个月的77.4%不等。除了SF-36一个子量表中的两项特定时间测量外,LC和SIC之间没有差异。在所有三份问卷中,比较微创手术和中转手术的几个子量表存在显著差异。
采用适当的方法学质量和循证指南(使用SF-36和GIQLI),LC和SIC在健康状况方面没有显著差异。