Breen Ronan A M, Hardy Gareth A D, Perrin Felicity M R, Lear Sara, Kinloch Sabine, Smith Colette J, Cropley Ian, Janossy George, Lipman Marc C I
Department of Immunology, Royal Free & University College Medical School, London, United Kingdom.
PLoS One. 2007 Dec 19;2(12):e1335. doi: 10.1371/journal.pone.0001335.
Blood-based studies have demonstrated the potential of immunological assays to detect tuberculosis. However lung fluid sampling may prove superior as it enables simultaneous microbiological detection of mycobacteria to be performed. Until now this has only been possible using the expensive and invasive technique of broncho-alveolar lavage. We sought to evaluate an immunoassay using non-invasive induced-sputum to diagnose active tuberculosis.
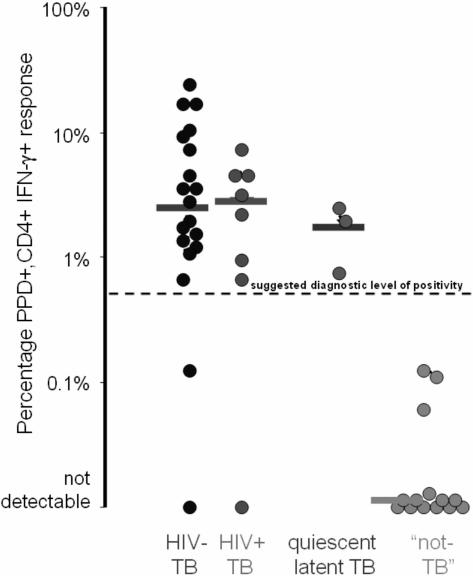
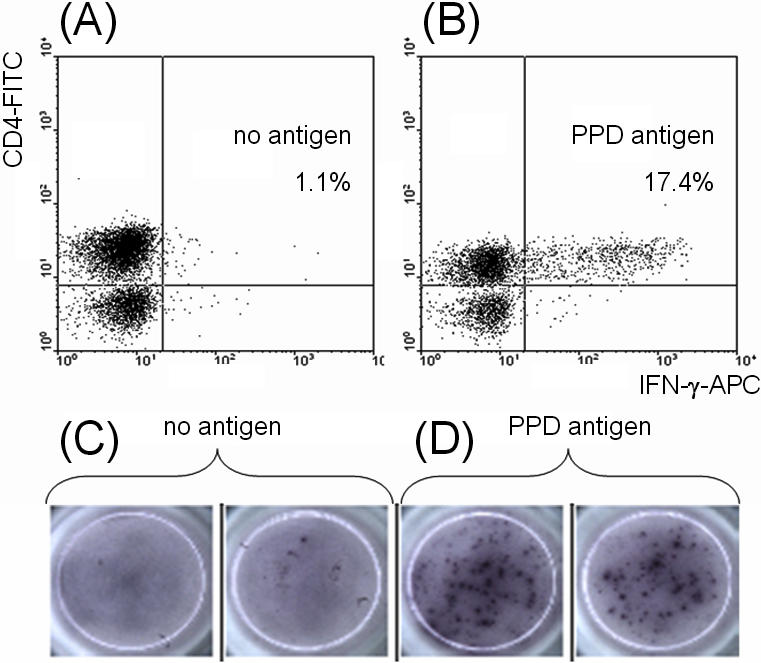
Prospective cohort study of forty-two spontaneous sputum smear-negative or sputum non-producing adults under investigation for tuberculosis. CD4 lymphocytes specific to purified-protein-derivative of Mycobacterium tuberculosis actively synthesising interferon-gamma were measured by flow cytometry and final diagnosis compared to immunoassay using a cut-off of 0.5%. Sixteen subjects (38%) were HIV-infected (median CD4 count [range] = 332 cells/microl [103-748]). Thirty-eight (90%) were BCG-vaccinated. In 27 subjects diagnosed with active tuberculosis, the median [range] percentage of interferon-gamma synthetic CD4+ lymphocytes was 2.77% [0-23.93%] versus 0% [0-2.10%] in 15 negative for active infection (p<0.0001). Sensitivity and specificity of the immunoassay versus final diagnosis of active tuberculosis were 89% (24 of 27) and 80% (12 of 15) respectively. The 3 positive assays in the latter group occurred in subjects diagnosed with quiescent/latent tuberculosis. Assay performance was unaffected by HIV-status, BCG-vaccination or disease site. Combining this approach with traditional microbiological methods increased the diagnostic yield to 93% (25 of 27) alongside acid-fast bacilli smear and 96% (26 of 27) alongside tuberculosis culture.
These data demonstrate for the first time that a rapid immunological assay to diagnose active tuberculosis can be performed successfully in combination with microbiological methods on a single induced-sputum sample.
基于血液的研究已证明免疫测定法在检测结核病方面的潜力。然而,肺液采样可能更具优势,因为它能够同时进行分枝杆菌的微生物学检测。到目前为止,这只能通过昂贵且具有侵入性的支气管肺泡灌洗技术来实现。我们试图评估一种使用无创诱导痰来诊断活动性结核病的免疫测定法。
对42名正在接受结核病调查的自发性痰涂片阴性或无痰的成年人进行前瞻性队列研究。通过流式细胞术测量对结核分枝杆菌纯化蛋白衍生物有特异性且能积极合成γ干扰素的CD4淋巴细胞,并将最终诊断结果与使用0.5%的临界值的免疫测定法进行比较。16名受试者(38%)感染了HIV(CD4细胞计数中位数[范围]=332个/微升[103 - 748])。38名(90%)接种过卡介苗。在27名被诊断为活动性结核病的受试者中,合成γ干扰素的CD4 +淋巴细胞的中位数[范围]百分比为2.77%[0 - 23.93%],而在15名活动性感染阴性的受试者中为0%[0 - 2.10%](p<0.0001)。免疫测定法相对于活动性结核病最终诊断的敏感性和特异性分别为89%(27例中的24例)和80%(15例中的12例)。后一组中的3例假阳性检测出现在被诊断为静止/潜伏性结核病的受试者中。检测性能不受HIV感染状态、卡介苗接种情况或疾病部位的影响。将这种方法与传统微生物学方法相结合,与抗酸杆菌涂片相比,诊断率提高到93%(27例中的25例),与结核培养相比,诊断率提高到96%(27例中的26例)。
这些数据首次证明,一种用于诊断活动性结核病的快速免疫测定法可以与微生物学方法成功结合,在单个诱导痰样本上进行检测。