Kalso Eija, Simpson Karen H, Slappendel Robert, Dejonckheere Joachim, Richarz Ute
Pain Clinic, Helsinki University Central Hospital, Helsinki, Finland.
BMC Med. 2007 Dec 21;5:39. doi: 10.1186/1741-7015-5-39.
Some patients with long-standing low back pain will benefit from treatment with strong opioids. However, it would be helpful to predict which patients will have a good response. A fixed-term opioid trial has been recommended, but there is little evidence to suggest how long this trial should be. We assessed data from a large-scale randomized comparison of transdermal fentanyl (TDF) and sustained-release oral morphine (slow-release morphine; SRM) to determine characteristics of treatment responders.
This was a secondary analysis of a previously published 13-month randomized trial involving 680 patients with long-standing low back pain (median age 52 years, 61% women, median duration of back pain 87 months). Pain relief was recorded using visual analogue scales (VAS). Treatment response was defined as pain relief of at least 30% from baseline to any point during the trial. We used a step-wise logistic regression to identify variables that might predict response to treatment. Covariates included treatment group, sex, age, duration of pain, presence of neuropathic pain, baseline pain scores, educational/employment status, use of high doses of opioids, and social functioning (SF)-36 scores.
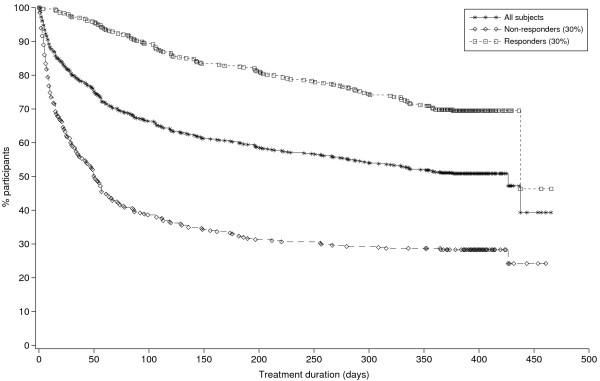
Over half the patients in both groups (n = 370; 54% TDF, 55% SRM) were treatment responders. There were no differences between the TDF and SRM responders in terms of age, sex, type or duration of pain between responders and non-responders. The difference in response to treatment between responders and non-responders could be detected at 3 weeks. Lack of response after 1 month had a stronger negative predictive value (i.e., ability to detect non-responders) than the presence of response after 1 month. The most influential factors for predicting a response were employment status (chi2 = 11.06, p = 0.0259) and use of high doses of opioids (chi2 = 3.04, p = 0.0811).
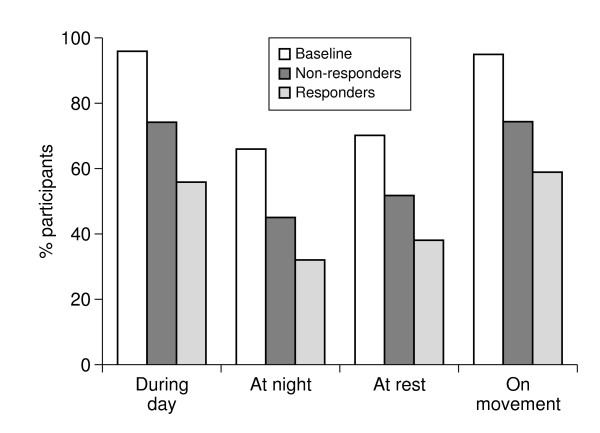
No clear pattern of baseline pain (type or severity) or patient characteristics emerged that could be used to predict responders before the start of opioid treatment. However, a 1-month trial period appears sufficient to determine response and tolerability in most cases.
一些长期患有腰痛的患者将从强效阿片类药物治疗中获益。然而,预测哪些患者会有良好反应将很有帮助。已推荐进行定期阿片类药物试验,但几乎没有证据表明该试验应持续多长时间。我们评估了一项关于透皮芬太尼(TDF)和缓释口服吗啡(缓释吗啡;SRM)的大规模随机对照试验的数据,以确定治疗反应者的特征。
这是对一项先前发表的为期13个月的随机试验的二次分析,该试验涉及680例长期腰痛患者(中位年龄52岁,61%为女性,腰痛中位持续时间87个月)。使用视觉模拟量表(VAS)记录疼痛缓解情况。治疗反应定义为从基线到试验期间任何时间点疼痛缓解至少30%。我们使用逐步逻辑回归来确定可能预测治疗反应的变量。协变量包括治疗组、性别、年龄、疼痛持续时间、是否存在神经性疼痛、基线疼痛评分、教育/就业状况、高剂量阿片类药物的使用以及社会功能(SF)-36评分。
两组中超过一半的患者(n = 370;TDF组为54%,SRM组为55%)是治疗反应者。TDF组和SRM组的反应者在年龄、性别、疼痛类型或持续时间方面,反应者与无反应者之间没有差异。在3周时可以检测到反应者与无反应者在治疗反应上的差异。1个月后无反应比1个月后有反应具有更强的阴性预测价值(即检测无反应者的能力)。预测反应的最有影响因素是就业状况(卡方 = 11.06,p = 0.0259)和高剂量阿片类药物的使用(卡方 = 3.04, p = 0.0811)。
在阿片类药物治疗开始前,没有出现可用于预测反应者的明确的基线疼痛模式(类型或严重程度)或患者特征。然而,在大多数情况下,1个月的试验期似乎足以确定反应和耐受性。