Eddleston Michael, Juszczak Edmund, Buckley Nick A, Senarathna Lalith, Mohamed Fahim, Dissanayake Wasantha, Hittarage Ariyasena, Azher Shifa, Jeganathan K, Jayamanne Shaluka, Sheriff Mh Rezvi, Warrell David A
Centre for Tropical Medicine, Nuffield Department of Clinical Medicine, University of Oxford, Oxford, UK.
Lancet. 2008 Feb 16;371(9612):579-87. doi: 10.1016/S0140-6736(08)60270-6.
The case-fatality for intentional self-poisoning in the rural developing world is 10-50-fold higher than that in industrialised countries, mostly because of the use of highly toxic pesticides and plants. We therefore aimed to assess whether routine treatment with multiple-dose activated charcoal, to interrupt enterovascular or enterohepatic circulations, offers benefit compared with no charcoal in such an environment.
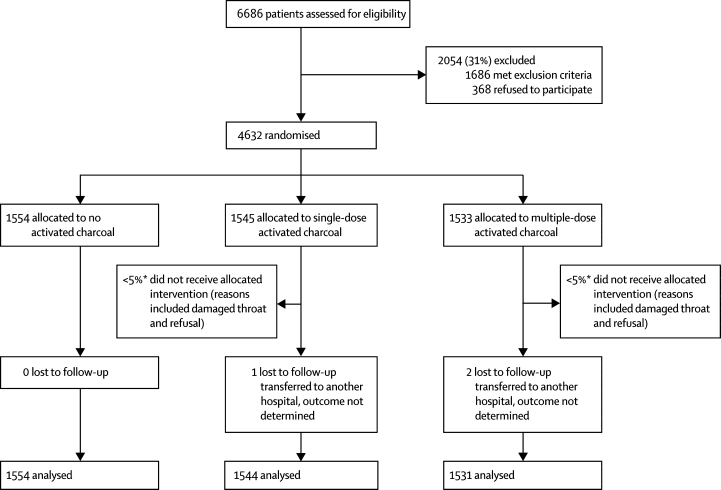
We did an open-label, parallel group, randomised, controlled trial of six 50 g doses of activated charcoal at 4-h intervals versus no charcoal versus one 50 g dose of activated charcoal in three Sri Lankan hospitals. 4632 patients were randomised to receive no charcoal (n=1554), one dose of charcoal (n=1545), or six doses of charcoal (n=1533); outcomes were available for 4629 patients. 2338 (51%) individuals had ingested pesticides, whereas 1647 (36%) had ingested yellow oleander (Thevetia peruviana) seeds. Mortality was the primary outcome measure. Analysis was by intention to treat. The trial is registered with controlled-trials.com as ISRCTN02920054.
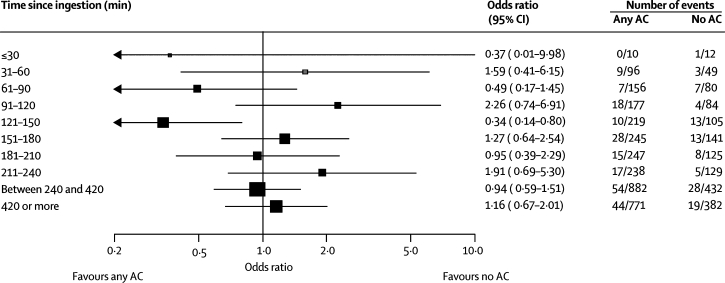
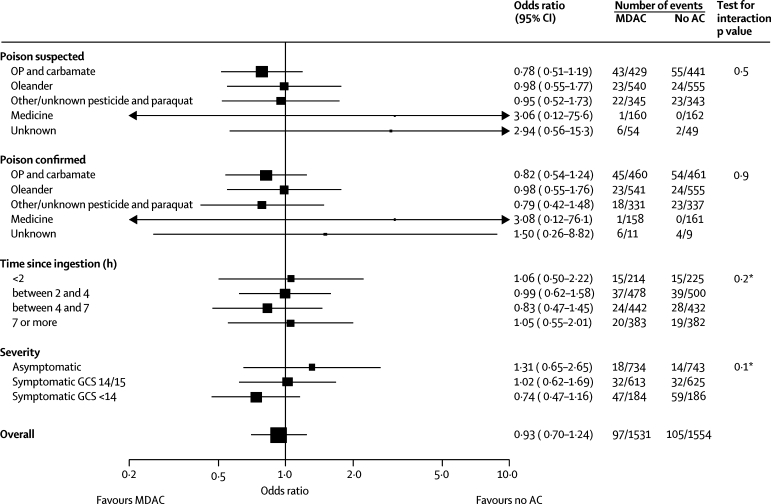
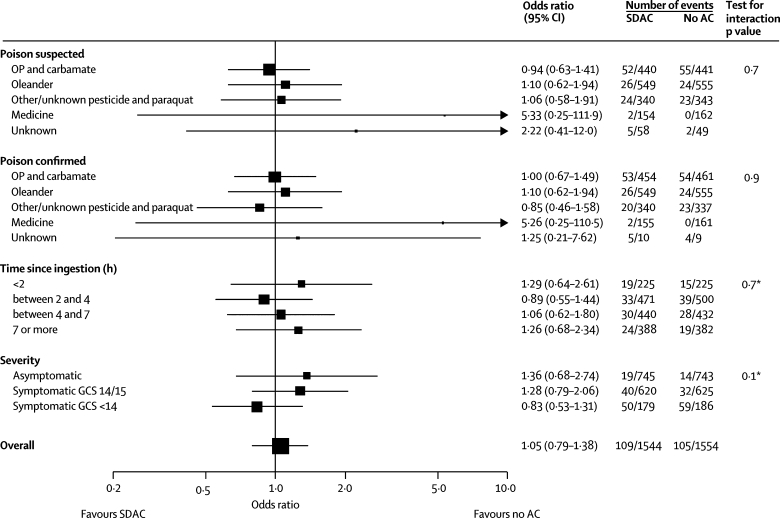
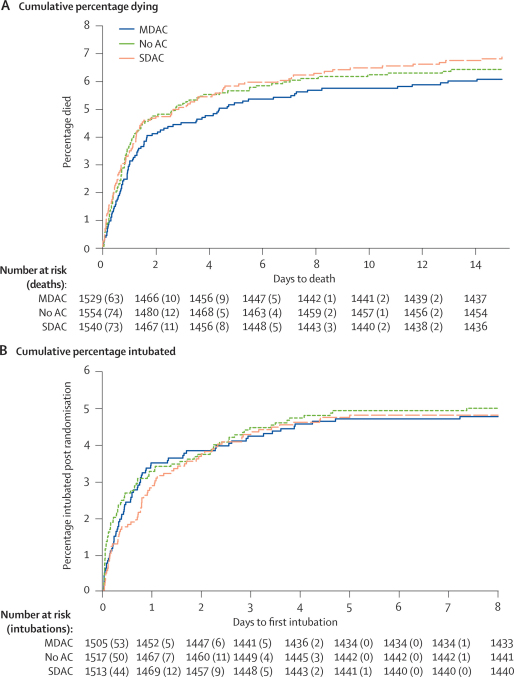
Mortality did not differ between the groups. 97 (6.3%) of 1531 participants in the multiple-dose group died, compared with 105 (6.8%) of 1554 in the no charcoal group (adjusted odds ratio 0.96, 95% CI 0.70-1.33). No differences were noted for patients who took particular poisons, were severely ill on admission, or who presented early.
We cannot recommend the routine use of multiple-dose activated charcoal in rural Asia Pacific; although further studies of early charcoal administration might be useful, effective affordable treatments are urgently needed.
在农村发展中地区,故意自我中毒的病死率比工业化国家高10至50倍,主要原因是使用了剧毒农药和植物。因此,我们旨在评估在这种环境下,采用多剂量活性炭进行常规治疗以中断肠血管或肠肝循环,与不使用活性炭相比是否有益。
我们在斯里兰卡的三家医院进行了一项开放标签、平行组、随机对照试验,比较每4小时服用六剂50克活性炭与不服用活性炭以及服用一剂50克活性炭的效果。4632名患者被随机分为不服用活性炭组(n = 1554)、服用一剂活性炭组(n = 1545)或服用六剂活性炭组(n = 1533);4629名患者有可用的结局数据。2338名(51%)个体摄入了农药,而1647名(36%)摄入了黄花夹竹桃种子。死亡率是主要结局指标。分析采用意向性分析。该试验在controlled-trials.com上注册,注册号为ISRCTN02920054。
各组之间的死亡率没有差异。多剂量组1531名参与者中有97名(6.3%)死亡,不服用活性炭组1554名中有105名(6.8%)死亡(调整后的优势比为0.96,95%置信区间为0.70 - 1.33)。对于摄入特定毒物、入院时病情严重或就诊较早的患者,未发现差异。
我们不建议在亚太农村地区常规使用多剂量活性炭;尽管对早期使用活性炭进行进一步研究可能有用,但迫切需要有效且负担得起的治疗方法。