Paul Friedemann, Waiczies Sonia, Wuerfel Jens, Bellmann-Strobl Judith, Dörr Jan, Waiczies Helmar, Haertle Mareile, Wernecke Klaus D, Volk Hans-Dieter, Aktas Orhan, Zipp Frauke
Cecilie Vogt Clinic for Neurology in the HELIOS Clinic Berlin-Buch, Charité-University Medicine Berlin and Max-Delbrueck Center for Molecular Medicine, Berlin, Germany.
PLoS One. 2008 Apr 9;3(4):e1928. doi: 10.1371/journal.pone.0001928.
Recent data from animal models of multiple sclerosis (MS) and from a pilot study indicated a possible beneficial impact of statins on MS.
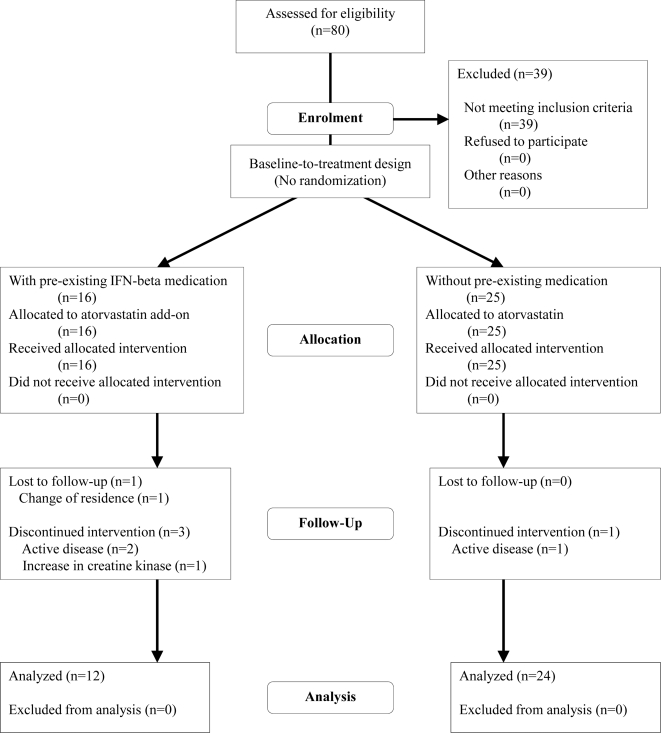
METHODOLOGY/PRINCIPAL FINDINGS: Safety, tolerability and effects on disease activity of atorvastatin given alone or in combination with interferon-beta (IFN-beta) were assessed in a phase II open-label baseline-to-treatment trial in relapsing-remitting MS (RRMS). Patients with at least one gadolinium-enhancing lesion (CEL) at screening by magnetic resonance imaging (MRI) were eligible for the study. After a baseline period of 3 monthly MRI scans (months -2 to 0), patients followed a 9-month treatment period on 80 mg atorvastatin daily. The number of CEL in treatment months 6 to 9 compared to baseline served as the primary endpoint. Other MRI-based parameters as well as changes in clinical scores and immune responses served as secondary endpoints. Of 80 RRMS patients screened, 41 were included, among them 16 with IFN-beta comedication. The high dose of 80 mg atorvastatin was well tolerated in the majority of patients, regardless of IFN-beta comedication. Atorvastatin treatment led to a substantial reduction in the number and volume of CEL in two-sided multivariate analysis (p = 0.003 and p = 0.008). A trend towards a significant decrease in number and volume of CEL was also detected in patients with IFN-beta comedication (p = 0.060 and p = 0.062), in contrast to patients without IFN-beta comedication (p = 0.170 and p = 0.140). Immunological investigations showed no suppression in T cell response but a significant increase in IL-10 production.
CONCLUSIONS/SIGNIFICANCE: Our data suggest that high-dose atorvastatin treatment in RRMS is safe and well tolerated. Moreover, MRI analysis indicates a possible beneficial effect of atorvastatin, alone or in combination with IFN-beta, on the development of new CEL. Thus, our findings provide a rationale for phase II/III trials, including combination of atorvastatin with already approved immunomodulatory therapy regimens.
ClinicalTrials.gov NCT00616187.
来自多发性硬化症(MS)动物模型和一项初步研究的最新数据表明,他汀类药物可能对MS有有益影响。
方法/主要发现:在一项复发缓解型MS(RRMS)的II期开放标签基线至治疗试验中,评估了单独使用阿托伐他汀或与干扰素-β(IFN-β)联合使用时的安全性、耐受性以及对疾病活动的影响。通过磁共振成像(MRI)筛查时至少有一个钆增强病灶(CEL)的患者符合研究条件。在进行3次每月一次MRI扫描的基线期(-2至0个月)后,患者接受为期9个月的每日80毫克阿托伐他汀治疗。将治疗第6至9个月的CEL数量与基线相比作为主要终点。其他基于MRI的参数以及临床评分和免疫反应的变化作为次要终点。在80名接受筛查的RRMS患者中,41名被纳入研究,其中16名同时接受IFN-β治疗。无论是否同时接受IFN-β治疗,大多数患者对80毫克的高剂量阿托伐他汀耐受性良好。在双侧多变量分析中,阿托伐他汀治疗导致CEL数量和体积大幅减少(p = 0.003和p = 0.008)。与未同时接受IFN-β治疗的患者(p = 0.170和p = 0.140)相比,同时接受IFN-β治疗的患者在CEL数量和体积上也有显著减少的趋势(p = 0.060和p = 0.062)。免疫学研究显示T细胞反应未受抑制,但IL-10产生显著增加。
结论/意义:我们的数据表明,RRMS患者接受高剂量阿托伐他汀治疗是安全且耐受性良好的。此外,MRI分析表明阿托伐他汀单独或与IFN-β联合使用可能对新CEL的形成有有益作用。因此,我们的研究结果为II/III期试验提供了理论依据,包括阿托伐他汀与已批准的免疫调节治疗方案联合使用。
ClinicalTrials.gov NCT00616187。