Si Damin, Bailie Ross, Cunningham Joan, Robinson Gary, Dowden Michelle, Stewart Allison, Connors Christine, Weeramanthri Tarun
Menzies School of Health Research, Institute of Advanced Studies, Charles Darwin University, Darwin, NT, Australia.
BMC Health Serv Res. 2008 May 28;8:112. doi: 10.1186/1472-6963-8-112.
Indigenous Australians experience disproportionately high prevalence of, and morbidity and mortality from chronic illness such as diabetes, renal disease and cardiovascular disease. Improving the understanding of how Indigenous primary care systems are organised to deliver chronic illness care will inform efforts to improve the quality of care for Indigenous people.
This cross-sectional study was conducted in 12 Indigenous communities in Australia's Northern Territory. Using the Chronic Care Model as a framework, we carried out a mail-out survey to collect information on material, financial and human resources relating to chronic illness care in participating health centres. Follow up face-to-face interviews with health centre staff were conducted to identify successes and difficulties in the systems in relation to providing chronic illness care to community members.
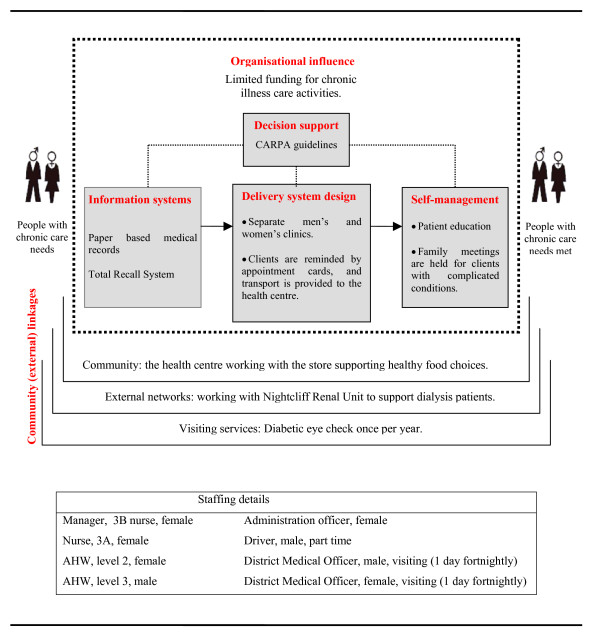
Participating health centres had distinct areas of strength and weakness in each component of systems: 1) organisational influence - strengthened by inclusion of chronic illness goals in business plans, appointment of designated chronic disease coordinators and introduction of external clinical audits, but weakened by lack of training in disease prevention and health promotion and limited access to Medicare funding; 2) community linkages - facilitated by working together with community organisations (e.g. local stores) and running community-based programs (e.g. "health week"), but detracted by a shortage of staff especially of Aboriginal health workers working in the community; 3) self management - promoted through patient education and goal setting with clients, but impeded by limited focus on family and community-based activities due to understaffing; 4) decision support - facilitated by distribution of clinical guidelines and their integration with daily care, but limited by inadequate access to and support from specialists; 5) delivery system design - strengthened by provision of transport for clients to health centres, separate men's and women's clinic rooms, specific roles of primary care team members in relation to chronic illness care, effective teamwork, and functional pathology and pharmacy systems, but weakened by staff shortage (particularly doctors and Aboriginal health workers) and high staff turnover; and 6) clinical information systems - facilitated by wide adoption of computerised information systems, but weakened by the systems' complexity and lack of IT maintenance and upgrade support.
Using concrete examples, this study translates the concept of the Chronic Care Model (and associated systems view) into practical application in Australian Indigenous primary care settings. This approach proved to be useful in understanding the quality of primary care systems for prevention and management of chronic illness. Further refinement of the systems should focus on both increasing human and financial resources and improving management practice.
澳大利亚原住民患糖尿病、肾病和心血管疾病等慢性病的比例、发病率和死亡率极高。深入了解原住民初级保健系统如何组织以提供慢性病护理,将为提高原住民护理质量的努力提供信息。
这项横断面研究在澳大利亚北领地的12个原住民社区进行。以慢性病护理模型为框架,我们开展了一项邮寄调查,以收集参与的健康中心与慢性病护理相关的物质、财务和人力资源信息。对健康中心工作人员进行后续面对面访谈,以确定该系统在为社区成员提供慢性病护理方面的成功经验和困难。
参与的健康中心在系统的每个组成部分都有明显的优势和劣势:1)组织影响力——通过在业务计划中纳入慢性病目标、任命指定的慢性病协调员和引入外部临床审计得到加强,但因缺乏疾病预防和健康促进培训以及医疗保险资金获取有限而减弱;2)社区联系——通过与社区组织(如当地商店)合作和开展社区项目(如“健康周”)得到促进,但因工作人员短缺,尤其是在社区工作的原住民卫生工作者短缺而受到影响;3)自我管理——通过对患者进行教育和与客户设定目标得到促进,但因人员不足导致对家庭和社区活动的关注有限而受到阻碍;4)决策支持——通过分发临床指南并将其与日常护理相结合得到促进,但因专科医生的获取和支持不足而受到限制;5)服务提供系统设计——通过为患者提供前往健康中心的交通、男女分开的诊疗室、初级保健团队成员在慢性病护理方面的特定角色、有效的团队合作以及功能完善的病理和药房系统得到加强,但因人员短缺(尤其是医生和原住民卫生工作者)和员工流动率高而减弱;6)临床信息系统——通过广泛采用计算机化信息系统得到促进,但因系统复杂以及缺乏信息技术维护和升级支持而减弱。
本研究通过具体实例,将慢性病护理模型的概念(以及相关的系统观点)转化为澳大利亚原住民初级保健环境中的实际应用。这种方法被证明有助于理解用于预防和管理慢性病的初级保健系统的质量。系统的进一步完善应侧重于增加人力和财力资源以及改进管理实践。