Bailie Ross, Si Damin, Dowden Michelle, O'Donoghue Lynette, Connors Christine, Robinson Gary, Cunningham Joan, Weeramanthri Tarun
Menzies School of Health Research, Institute of Advanced Studies, Charles Darwin University, Darwin, NT, Australia.
BMC Health Serv Res. 2007 May 6;7:67. doi: 10.1186/1472-6963-7-67.
Indigenous Australians experience disproportionately high prevalence of, and morbidity and mortality from diabetes. There is an urgent need to understand how Indigenous primary care systems are organised to deliver diabetes services to those most in need, to monitor the quality of diabetes care received by Indigenous people, and to improve systems for better diabetes care.
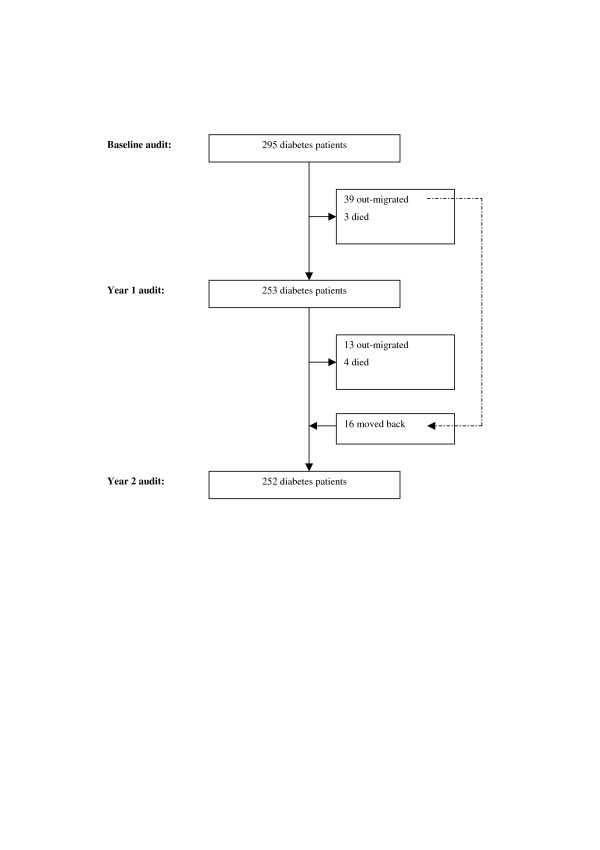
The intervention featured two annual cycles of assessment, feedback workshops, action planning, and implementation of system changes in 12 Indigenous community health centres. Assessment included a structured review of health service systems and audit of clinical records. Main process of care measures included adherence to guideline-scheduled services and medication adjustment. Main patient outcome measures were HbA1c, blood pressure and total cholesterol levels.
There was good engagement of health centre staff, with significant improvements in system development over the study period. Adherence to guideline-scheduled processes improved, including increases in 6 monthly testing of HbA1c from 41% to 74% (Risk ratio 1.93, 95% CI 1.71-2.10), 3 monthly checking of blood pressure from 63% to 76% (1.27, 1.13-1.37), annual testing of total cholesterol from 56% to 74% (1.36, 1.20-1.49), biennial eye checking by a ophthalmologist from 34% to 54% (1.68, 1.39-1.95), and 3 monthly feet checking from 20% to 58% (3.01, 2.52-3.47). Medication adjustment rates following identification of elevated HbA1c and blood pressure were low, increasing from 10% to 24%, and from 13% to 21% respectively at year 1 audit. However, improvements in medication adjustment were not maintained at the year 2 follow-up. Mean HbA1c value improved from 9.3 to 8.9% (mean difference -0.4%, 95% CI -0.7;-0.1), but there was no improvement in blood pressure or cholesterol control.
This quality improvement (QI) intervention has proved to be highly acceptable in the Indigenous Australian primary care setting and has been associated with significant improvements in systems and processes of care and some intermediate outcomes. However, improvements appear to be limited by inadequate attention to abnormal clinical findings and medication management. Greater improvement in intermediate outcomes may be achieved by specifically addressing system barriers to therapy intensification through more effective engagement of medical staff in QI activities and/or greater use of nurse-practitioners.
澳大利亚原住民糖尿病的患病率、发病率和死亡率极高。迫切需要了解原住民初级保健系统是如何组织的,以便为最需要的人群提供糖尿病服务,监测原住民接受糖尿病护理的质量,并改进系统以提供更好的糖尿病护理。
该干预措施包括在12个原住民社区卫生中心进行两个年度周期的评估、反馈研讨会、行动计划制定以及系统变革实施。评估包括对卫生服务系统的结构化审查和临床记录审计。主要护理过程指标包括遵循指南规定的服务和药物调整。主要患者结局指标为糖化血红蛋白(HbA1c)、血压和总胆固醇水平。
卫生中心工作人员积极参与,在研究期间系统发展有显著改善。遵循指南规定流程的情况有所改善,包括每6个月检测HbA1c的比例从41%增至74%(风险比1.93,95%置信区间1.71 - 2.10),每3个月检查血压的比例从63%增至76%(1.27,1.13 - 1.37),每年检测总胆固醇的比例从56%增至74%(1.36,1.20 - 1.49),每两年由眼科医生进行眼部检查的比例从34%增至54%(1.68,1.39 - 1.95),以及每3个月检查足部的比例从20%增至58%(3.01,2.52 - 3.47)。在第1年审计时,识别出HbA1c和血压升高后的药物调整率较低,分别从10%增至24%和从13%增至21%。然而,在第2年随访时药物调整的改善情况未得到维持。平均HbA1c值从9.3%降至8.9%(平均差值 -0.4%,95%置信区间 -0.7;-0.1),但血压或胆固醇控制情况无改善。
在澳大利亚原住民初级保健环境中,这种质量改进(QI)干预措施已被证明是高度可接受的,并且与护理系统和流程的显著改善以及一些中间结局相关。然而,改善似乎受到对异常临床发现和药物管理关注不足的限制。通过让医务人员更有效地参与QI活动和/或更多地使用执业护士来专门解决强化治疗的系统障碍,可能会在中间结局方面取得更大改善。