Bahwere Paluku, Piwoz Ellen, Joshua Marthias C, Sadler Kate, Grobler-Tanner Caroline H, Guerrero Saul, Collins Steve
Valid International, Unit 9, Standingford House, 26 Cave Street, Oxford, OX4 1BA, UK.
BMC Infect Dis. 2008 Jul 31;8:106. doi: 10.1186/1471-2334-8-106.
In Malawi and other high HIV prevalence countries, studies suggest that more than 30% of all severely malnourished children admitted to inpatient nutrition rehabilitation units are HIV-infected. However, clinical algorithms designed to diagnose paediatric HIV are neither sensitive nor specific in severely malnourished children. The present study was conducted to assess : i) whether HIV testing can be integrated into Community-based Therapeutic Care (CTC); ii) to determine if CTC can improve the identification of HIV infected children; and iii) to assess the impact of CTC programmes on the rehabilitation of HIV-infected children with Severe Acute Malnutrition (SAM).
This community-based cohort study was conducted in Dowa District, Central Malawi, a rural area 50 km from the capital, Lilongwe. Caregivers and children admitted in the Dowa CTC programme were prospectively (Prospective Cohort = PC) and retrospectively (Retrospective Cohort = RC) admitted into the study and offered HIV testing and counseling. Basic medical care and community nutrition rehabilitation was provided for children with SAM. The outcomes of interest were uptake of HIV testing, and recovery, relapse, and growth rates of HIV-positive and uninfected children in the CTC programme. Student's t-test and analysis of variance were used to compare means and Kruskall Wallis tests were used to compare medians. Dichotomous variables were compared using Chi2 analyses and Fisher's exact test. Stepwise logistic regression with backward elimination was used to identify predictors of HIV infection (alpha = 0.05).
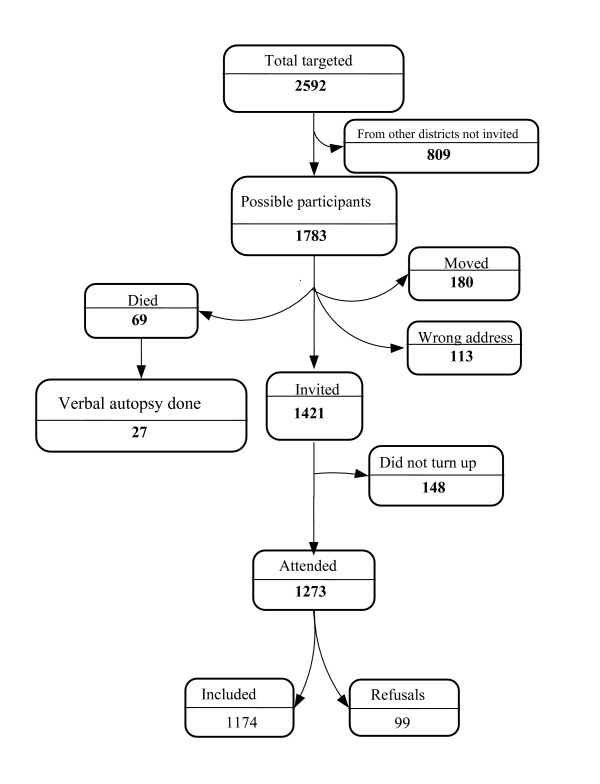
1273 and 735 children were enrolled in the RC and PC. For the RC, the average age (SD) at CTC admission was 30.0 (17.2) months. For the PC, the average age at admission was 26.5 (13.7) months. Overall uptake of HIV testing was 60.7% for parents and 94% for children. HIV prevalence in severely malnourished children was 3%, much lower than anticipated. 59% of HIV-positive and 83% of HIV-negative children achieved discharge Weight-For-Height (WFH) > or = 80% of the NCHS reference median (p = 0.003). Clinical algorithms for diagnosing HIV in SAM children had poor sensitivity and specificity.
CTC is a potentially valuable entry point for providing HIV testing and care in the community to HIV infected children with SAM.
在马拉维和其他艾滋病毒高流行率国家,研究表明,入住住院营养康复单位的所有重度营养不良儿童中,超过30%感染了艾滋病毒。然而,旨在诊断儿童艾滋病毒的临床算法在重度营养不良儿童中既不敏感也不特异。本研究旨在评估:i)艾滋病毒检测是否可以纳入社区治疗护理(CTC);ii)确定CTC是否可以改善对艾滋病毒感染儿童的识别;iii)评估CTC项目对患有严重急性营养不良(SAM)的艾滋病毒感染儿童康复的影响。
这项基于社区的队列研究在马拉维中部的多瓦区进行,该地区是一个距首都利隆圭50公里的农村地区。参与多瓦CTC项目的照顾者和儿童被前瞻性地(前瞻性队列=PC)和回顾性地(回顾性队列=RC)纳入研究,并接受艾滋病毒检测和咨询。为患有SAM的儿童提供基本医疗护理和社区营养康复。感兴趣的结果是艾滋病毒检测的接受情况,以及CTC项目中艾滋病毒阳性和未感染儿童的康复、复发和生长率。使用学生t检验和方差分析比较均值,使用克鲁斯卡尔-沃利斯检验比较中位数。使用卡方分析和费舍尔精确检验比较二分变量。使用向后消除的逐步逻辑回归来确定艾滋病毒感染的预测因素(α=0.05)。
RC组和PC组分别有1273名和735名儿童入组。对于RC组,CTC入院时的平均年龄(标准差)为30.0(17.2)个月。对于PC组,入院时的平均年龄为26.5(13.7)个月。家长对艾滋病毒检测的总体接受率为60.7%,儿童为94%。重度营养不良儿童中的艾滋病毒流行率为3%,远低于预期。59%的艾滋病毒阳性儿童和83%的艾滋病毒阴性儿童出院时的身高体重比(WFH)≥美国国家卫生统计中心参考中位数的80%(p=0.003)。用于诊断SAM儿童艾滋病毒的临床算法敏感性和特异性较差。
CTC是在社区为患有SAM的艾滋病毒感染儿童提供艾滋病毒检测和护理的一个潜在有价值的切入点。