Nazir Sarfraz Ahmed, Raza Syed Arsalan, Nazir Sheraz, Sherwood William, Bowker Colene, Lakhoo Kokila
Department of Radiology, John Radcliffe Hospital, Oxford, UK.
J Med Case Rep. 2008 Aug 1;2:256. doi: 10.1186/1752-1947-2-256.
Cystic hygroma is a benign congenital neoplasm that mostly presents as a soft-tissue mass in the posterior triangle of the neck. Pure mediastinal lesions are uncommon; the vast majority are asymptomatic and are an incidental finding in adulthood. The diagnosis is often made intra- or postoperatively. Prenatal identification is exceptional and post-natal diagnosis also proves challenging.
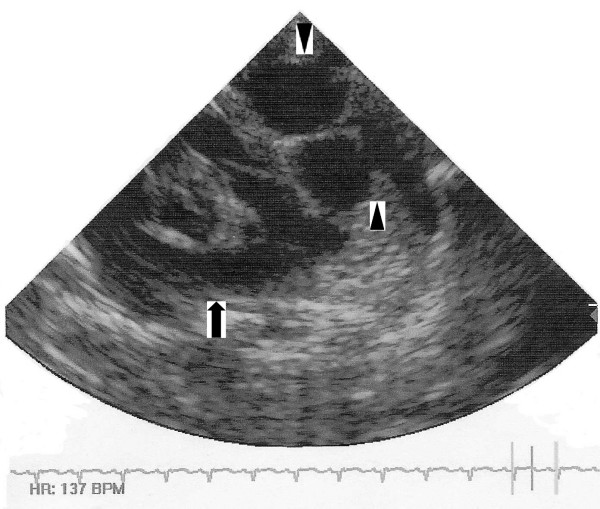
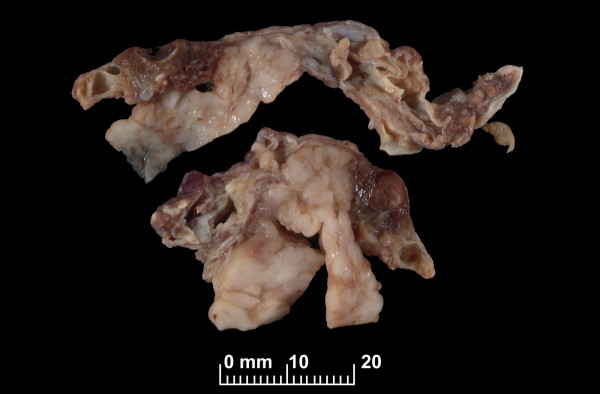
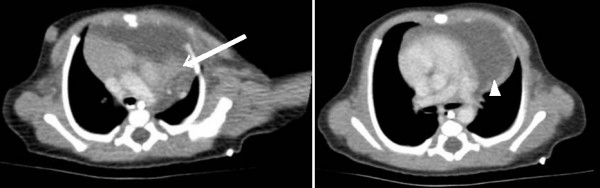
We report one such case that was mistaken for other entities in both the prenatal and immediate post-natal period. Initial and follow-up antenatal ultrasound scans demonstrated a multicystic lesion in the left chest, and the mother was counselled about the possibility of her baby having a congenital diaphragmatic hernia. Initial post-natal chest radiographs were reported as normal. An echocardiogram and thoracic computed tomography scan confirmed a complex multiloculated cystic mediastinal mass. The working diagnoses were of a mediastinal teratoma or congenital cystic adenomatous malformation. At operation, the lesion was compressed by the left lung and was found to be close to the left phrenic nerve, which was carefully identified and preserved. After excision, histopathological examination of the mass confirmed the diagnosis of cystic hygroma. Postoperative dyspnoea was observed secondary to paradoxical movement of the left hemidiaphragm and probable left phrenic neuropraxia. This settled conservatively with excellent recovery.
Despite the fact that isolated intrathoracic cystic hygroma is a rare entity, it needs to be considered in the differential diagnosis of foetal and neonatal mediastinal masses, particularly for juxtadiaphragmatic lesions. The phrenic nerve is not identifiable on prenatal ultrasound imaging, and it is therefore understandable that a mass close to the diaphragm may be mistaken for a congenital diaphragmatic hernia because of the location, morphology and potential phrenic nerve compression. Post-natal diagnosis may also be misleading as many mediastinal cystic masses have similar appearances on imaging. Therefore, as well as cystic architecture, special consideration needs to be given to the anatomical location and effect on local structures.
囊状水瘤是一种良性先天性肿瘤,多表现为颈部后三角区的软组织肿块。单纯纵隔病变并不常见;绝大多数无症状,在成年期偶然发现。诊断通常在术中或术后做出。产前识别极为罕见,产后诊断也颇具挑战性。
我们报告了这样一例在产前及产后即刻均被误诊为其他疾病的病例。初次及后续产前超声检查显示左胸有一多房性病变,医生告知母亲其婴儿可能患有先天性膈疝。产后初次胸部X线片报告正常。超声心动图和胸部计算机断层扫描证实为复杂的多房性纵隔囊性肿块。初步诊断为纵隔畸胎瘤或先天性囊性腺瘤样畸形。手术中,病变被左肺压迫,发现其靠近左膈神经,遂小心识别并予以保留。切除后,肿块的组织病理学检查确诊为囊状水瘤。术后观察到因左半膈矛盾运动及可能的左膈神经失用导致呼吸困难。经保守治疗后症状缓解,恢复良好。
尽管孤立性胸腔内囊状水瘤是一种罕见疾病,但在胎儿及新生儿纵隔肿块的鉴别诊断中仍需考虑,尤其是对于膈旁病变。产前超声成像无法识别膈神经,因此,由于位置、形态及可能的膈神经受压,靠近膈肌的肿块可能被误诊为先天性膈疝也就不难理解了。产后诊断也可能产生误导,因为许多纵隔囊性肿块在影像学上有相似表现。因此,除了囊性结构外,还需特别考虑解剖位置及对局部结构的影响。