Shipman Cathy, Gysels Marjolein, White Patrick, Worth Allison, Murray Scott A, Barclay Stephen, Forrest Sarah, Shepherd Jonathan, Dale Jeremy, Dewar Steve, Peters Marilyn, White Suzanne, Richardson Alison, Lorenz Karl, Koffman Jonathan, Higginson Irene J
King's College London, Department of Palliative Care, Policy and Rehabilitation, Weston Education Centre, London SE5 9RJ.
BMJ. 2008 Oct 1;337:a1720. doi: 10.1136/bmj.a1720.
To identify major concerns of national and local importance in the provision, commissioning, research, and use of generalist end of life care.
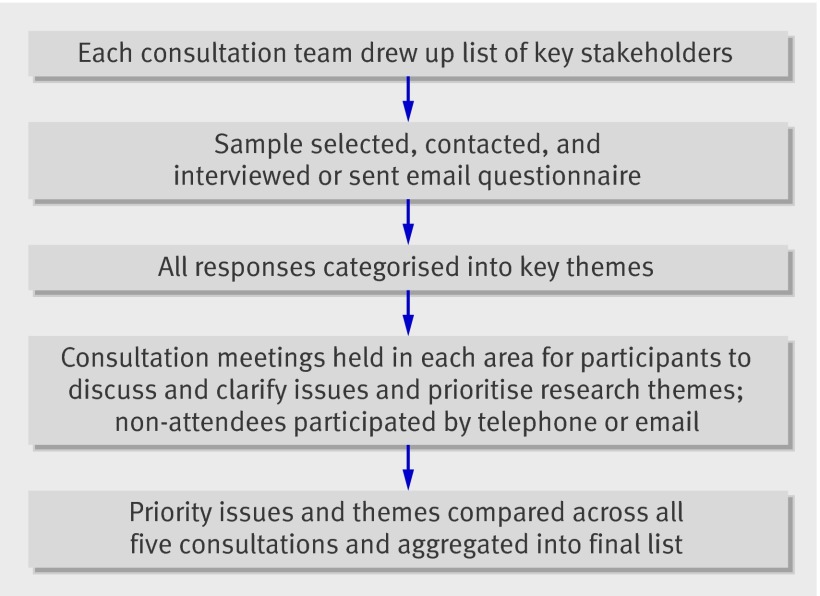
A national consultation and prioritising exercise using a modified form of the nominal group technique.
Healthcare practitioners, commissioners, academics, and representatives of user and voluntary groups.
Primary and secondary care, specialist palliative care, and academic and voluntary sectors in England and Scotland.
74% of those invited (210/285) participated. The stage of life to which "end of life care" referred was not understood in a uniform way. Perceptions ranged from a period of more than a year to the last few days of life. Prominent concerns included difficulties in prognosis and the availability of adequate support for patients with advanced non-malignant disease. Generalists in both primary and secondary care were usually caring for only a few patients approaching the end of life at any one time at a point in time. It was therefore challenging to maintain skills and expertise particularly as educational opportunities were often limited. End of life care took place among many other competing and incentivised activities for general practitioners in the community. More needs to be known about models of end of life care and how these can be integrated in a generalist's workload. A greater evidence base is needed about the effectiveness and application of current tools such as the gold standards framework and Liverpool care pathway and about models of palliation in patients with diseases other than cancer.
Definitions of end of life care need clarification and standardisation. A greater evidence base is needed to define models of good practice together with a commitment to provide education and training and adequate resources for service provision. More needs to be known about the context of provision and the influence of competing priorities and incentives.
确定在提供、委托开展、研究和使用全科临终关怀方面具有国家和地方重要性的主要关注点。
采用改良的名义群体技术进行全国性咨询和优先事项确定活动。
医疗从业者、委托方、学者以及用户和志愿团体的代表。
英格兰和苏格兰的初级和二级医疗、专科姑息治疗以及学术和志愿部门。
74%的受邀者(210/285)参与了活动。对于“临终关怀”所指的生命阶段,人们的理解并不统一。认知范围从一年多到生命的最后几天不等。突出的关注点包括预后困难以及为晚期非恶性疾病患者提供充分支持的可及性。在任何一个时间点,初级和二级医疗中的全科医生通常一次仅照顾少数临近生命终点的患者。因此,维持技能和专业知识具有挑战性,尤其是因为教育机会往往有限。在社区中,全科医生面临着许多其他相互竞争且有激励措施的活动,临终关怀就在这些活动之中。对于临终关怀模式以及如何将这些模式整合到全科医生的工作量中,我们还需要了解更多。对于当前工具(如黄金标准框架和利物浦护理路径)的有效性和应用以及非癌症疾病患者的姑息治疗模式,需要更多的证据基础。
临终关怀的定义需要澄清和标准化。需要更多的证据基础来定义良好实践模式,并承诺提供教育和培训以及充足的服务提供资源。我们还需要更多地了解服务提供的背景以及相互竞争的优先事项和激励措施的影响。