Plein Sven, Schwitter Juerg, Suerder Daniel, Greenwood John P, Boesiger Peter, Kozerke Sebastian
Institute for Biomedical Engineering, University and ETH Zurich, Zurich, Switzerland.
Radiology. 2008 Nov;249(2):493-500. doi: 10.1148/radiol.2492080017.
To determine the feasibility and diagnostic accuracy of high-spatial-resolution myocardial perfusion magnetic resonance (MR) imaging at 3.0 T by using k-space and time (k-t) domain undersampling with sensitivity encoding (SENSE), or k-t SENSE. Data were compared with results of k-t SENSE-accelerated high-spatial-resolution perfusion MR imaging at 1.5 T and standard-resolution acquisition at 3.0 T.
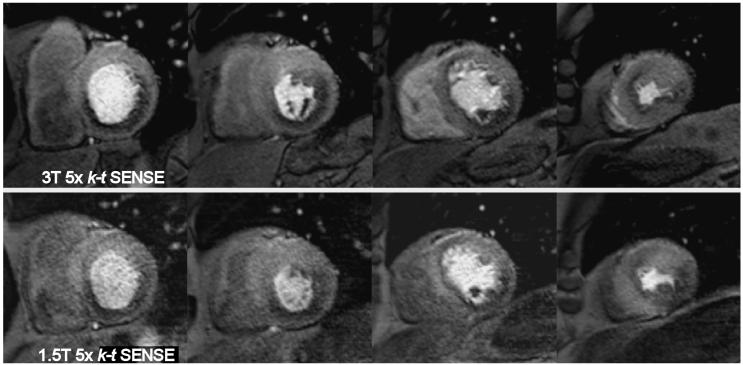
The study was reviewed and approved by the local ethics review board; informed consent was obtained. k-t SENSE perfusion MR imaging was performed at 1.5 and 3.0 T (fivefold k-t SENSE acceleration; spatial resolution, 1.3 x 1.3 x 10 mm). Fourteen volunteers were studied at rest; 37 patients were studied during adenosine-induced stress. In volunteers, comparison was also made with standard-resolution (2.5 x 2.5 x 10 mm) twofold SENSE perfusion MR imaging results at 3.0 T. Image quality, artifact scores, signal-to-noise ratios (SNRs), and contrast enhancement ratios were derived. In patients, diagnostic accuracy of visual analysis to detect stenosis of more than 50% narrowing in diameter at quantitative coronary angiography was determined by using receiver operator characteristic (ROC) analysis.
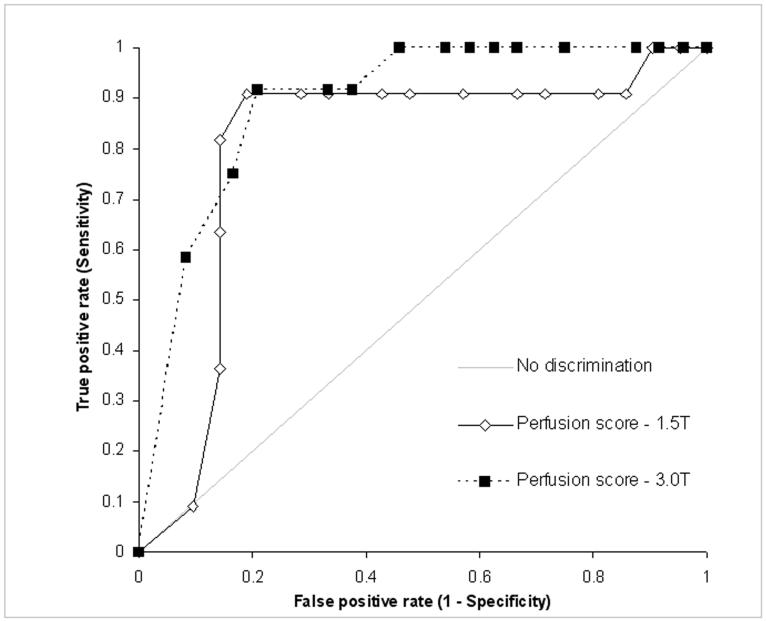
In volunteers, image quality and artifact scores were similar for 3.0- and 1.5-T k-t SENSE perfusion MR imaging, while SNR was higher (11.6 vs 5.6) and contrast enhancement ratio was lower (1.1 vs 1.5, P = .012) at 3.0 T. Compared with standard-resolution perfusion MR imaging, image quality was higher for 3.0-T k-t SENSE (3.6 vs 3.1, P = .04), endocardial dark rim artifacts were reduced (artifact thickness, 1.6 vs 2.4 mm, P < .001), and contrast enhancement ratios were similar. In patients, areas under the ROC curve for detection of coronary stenosis were 0.89 and 0.80 (P = .21) for 3.0 and 1.5 T, respectively.
k-t SENSE-accelerated high-spatial-resolution perfusion MR imaging at 3.0 T is feasible, with similar artifacts and diagnostic accuracy as those at 1.5 T. Compared with standard-resolution twofold SENSE perfusion MR imaging, image quality at k-t SENSE MR imaging is improved and artifacts are reduced.
通过使用带有灵敏度编码(SENSE)的k空间和时间(k-t)域欠采样技术(即k-t SENSE),确定3.0 T高空间分辨率心肌灌注磁共振(MR)成像的可行性和诊断准确性。将数据与1.5 T的k-t SENSE加速高空间分辨率灌注MR成像结果以及3.0 T的标准分辨率采集结果进行比较。
本研究经当地伦理审查委员会审核批准;获得了知情同意。在1.5 T和3.0 T进行k-t SENSE灌注MR成像(k-t SENSE加速五倍;空间分辨率为1.3×1.3×10 mm)。对14名志愿者进行静息状态研究;对37名患者进行腺苷诱导的负荷状态研究。在志愿者中,还将结果与3.0 T的标准分辨率(2.5×2.5×10 mm)两倍SENSE灌注MR成像结果进行比较。得出图像质量、伪影评分、信噪比(SNR)和对比增强率。在患者中,通过使用接受者操作特征(ROC)分析来确定视觉分析检测定量冠状动脉造影中直径狭窄超过50%的狭窄的诊断准确性。
在志愿者中,3.0 T和1.5 T的k-t SENSE灌注MR成像的图像质量和伪影评分相似,而3.0 T时的SNR更高(11.6对5.6),对比增强率更低(1.1对1.5,P = 0.012)。与标准分辨率灌注MR成像相比,3.0 T的k-t SENSE的图像质量更高(3.6对3.1,P = 0.04),心内膜暗边伪影减少(伪影厚度,1.6对2.4 mm,P < 0.001),对比增强率相似。在患者中,3.0 T和1.5 T检测冠状动脉狭窄的ROC曲线下面积分别为0.89和0.80(P = 0.21)。
3.0 T的k-t SENSE加速高空间分辨率灌注MR成像是可行的,其伪影和诊断准确性与1.5 T时相似。与标准分辨率两倍SENSE灌注MR成像相比,k-t SENSE MR成像的图像质量得到改善,伪影减少。