Butz Arlene M, Thompson Richard E, Tsoukleris Mona G, Donithan Michele, Hsu Van Doren, Mudd Kim, Zuckerman Ilene H, Bollinger Mary E
The Johns Hopkins University School of Medicine, Department of Pediatrics, Baltimore, MD 21287, USA.
J Asthma. 2008 Nov;45(9):800-6. doi: 10.1080/02770900802290697.
To determine whether temporal trends exist for short-acting beta agonist (SABA), oral corticosteroid (OCS), and anti-inflammatory prescription fills in children with persistent asthma.
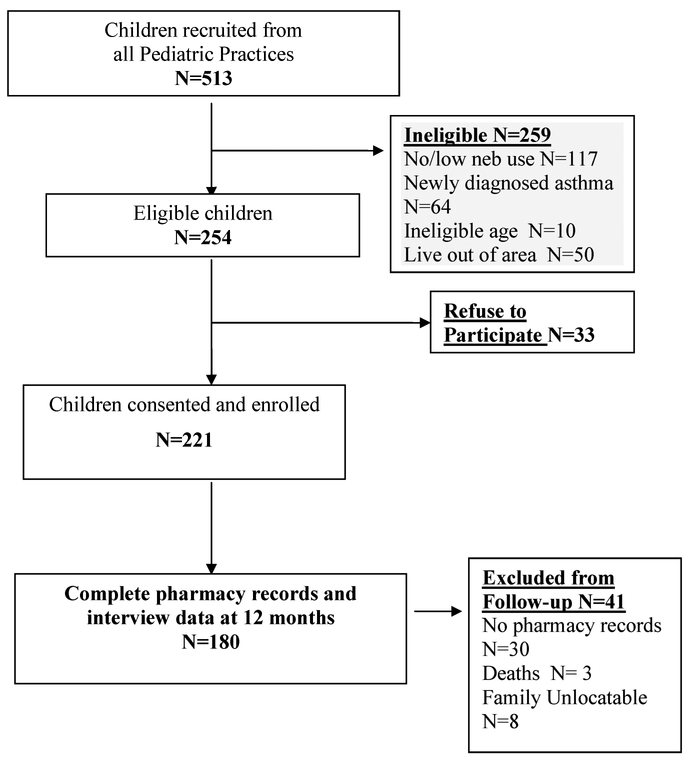
This was a longitudinal analysis of pharmacy record data and health information data obtained by parent report over 12 months for children with persistent asthma 2 to 9 years of age. Eligible children had to report current nebulizer use and one or more emergency department visits or hospitalizations within the past 12 months.
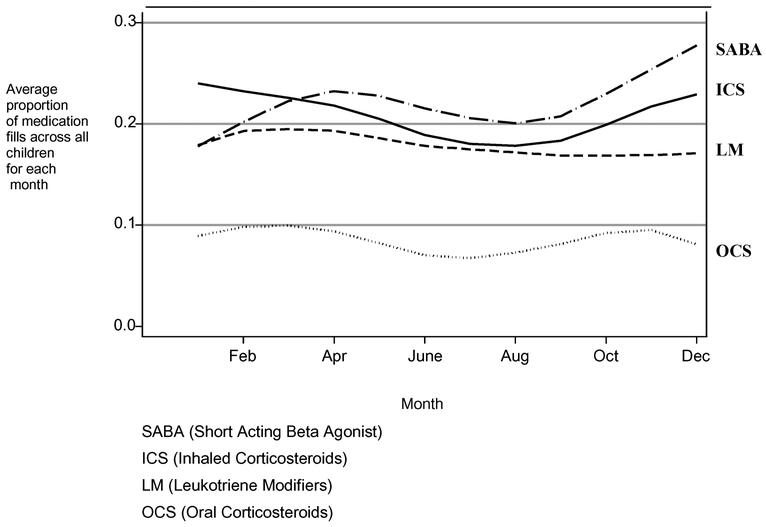
Children were primarily African-American (89%), male (64%), received Medicaid health insurance (82%), and were a mean age of 4.5 years (SD 2.1). Few families (11%) reported any problems paying for their child's asthma medications at baseline or at the 12-month follow-up. There was a high degree of association between filling a rescue (SABA or OCS) and controller (leukotriene modifier, inhaled corticosteroid, cromolyn) medication during the same month for all months with Pearson's correlation coefficients ranging from a low of 0.28 for October to a high of 0.53 in September. Short-acting beta agonist fills were significantly more likely to be filled concurrently with inhaled corticosteroid fills. However, significantly fewer prescription fills were obtained in the summer months with an acceleration of medication fills in September through December and an increase in early spring.
There was a summer decline in both inhaled corticosteroid and SABA fills. Timing of asthma monitoring visits to occur before peak prescription fill months, i.e., August and December for an asthma "tune-up," theoretically could improve asthma control. During these primary care visits children could benefit from more intensive monitoring of medication use including monitoring lung function, frequency of prescription refills, and assessment of medication device technique to ensure that an effective dose of medication is adequately delivered to the respiratory tract. Additionally, scheduling non-urgent asthma care visits at pre-peak prescription fill months can take advantage of "step down" during decreased symptom periods and when appropriate restart daily controller medications to "step up" prior to peak asthma periods.
确定持续性哮喘患儿使用短效β受体激动剂(SABA)、口服糖皮质激素(OCS)和抗炎药物处方的时间趋势是否存在。
这是一项对2至9岁持续性哮喘患儿12个月期间药房记录数据和家长报告获得的健康信息数据的纵向分析。符合条件的儿童必须报告当前使用雾化器情况以及在过去12个月内有一次或多次急诊就诊或住院情况。
儿童主要为非裔美国人(89%),男性(64%),接受医疗补助医疗保险(82%),平均年龄4.5岁(标准差2.1)。很少有家庭(11%)在基线或12个月随访时报告孩子哮喘药物支付有任何问题。在所有月份中,同一个月内开具急救(SABA或OCS)和控制药物(白三烯调节剂、吸入性糖皮质激素、色甘酸钠)之间存在高度相关性,皮尔逊相关系数从10月的低0.28到9月的高0.53不等。短效β受体激动剂处方更有可能与吸入性糖皮质激素处方同时开具。然而,夏季获得的处方明显较少,9月至12月药物处方加速,早春有所增加。
吸入性糖皮质激素和SABA处方量在夏季均有所下降。哮喘监测就诊时间安排在处方量高峰月份之前,即8月和12月进行哮喘“调整”,理论上可以改善哮喘控制。在这些初级保健就诊期间,儿童可以从更密集的药物使用监测中受益,包括监测肺功能、处方 refill频率以及评估药物装置技术,以确保有效剂量的药物充分输送到呼吸道。此外,在处方量高峰前的月份安排非紧急哮喘护理就诊,可以利用症状减轻期的“降级”,并在适当的时候在哮喘高峰期之前重新开始每日控制药物以“升级”。