BMJ. 2008 Oct 31;337:a1864. doi: 10.1136/bmj.a1864.
To systematically review fully randomised patient preference trials and to explore the impact of preferences on attrition and outcome by meta-analysis of patient level data.
Citation search using Science Citation Index and Google Scholar and search of the main electronic databases (Medline, CINAHL, Embase, and AMED) with a combination of key words.
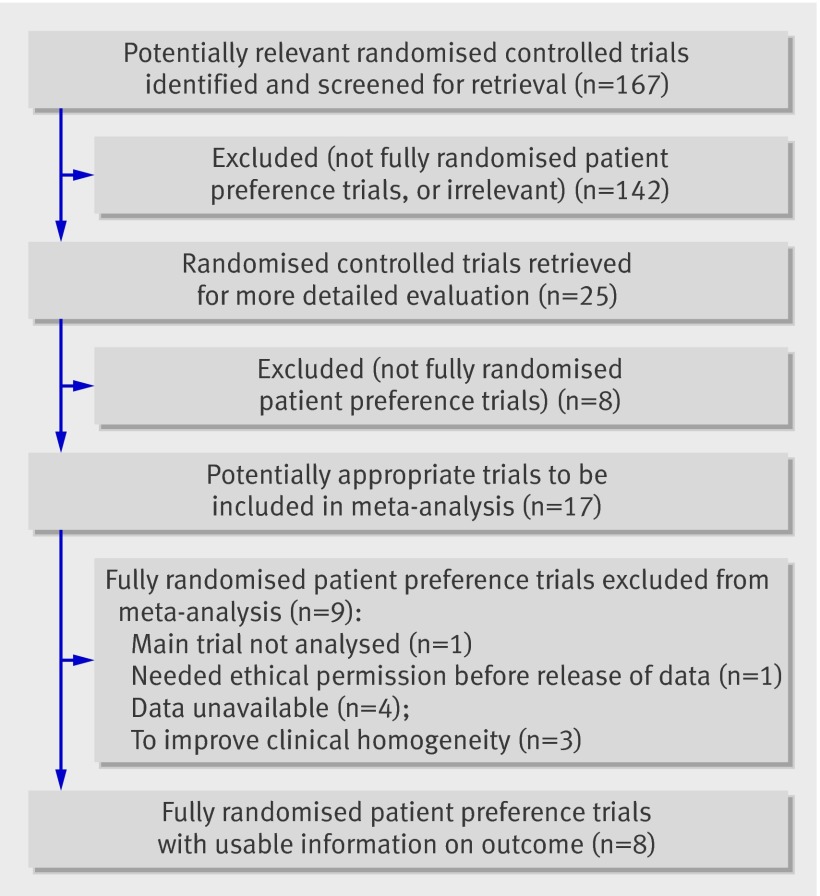
Fully randomised patient preference trials that compared treatments for any clinical condition were included. Other types of preference trials and crossover trials were excluded. Other inclusion criteria: participants aged 16 years and over; primary, self-reported outcomes measured on a continuous numerical scale. From 167 studies identified and screened, 17 were identified as fully randomised patient preference trials.
Of the 17 trials identified, 11 authors provided raw data for the meta-analysis. Data collected were baseline and follow-up data for the main outcome, randomised allocation data, preference data, and demographic data. Baseline and first post-intervention follow-up data for the main outcome were standardised. To improve homogeneity, data for only the eight musculoskeletal trials (n=1594) were combined. To estimate the effects of preferences on outcomes and attrition, three groups were compared: patients who had a preference and were randomly allocated to their preferred treatment; patients who had a preference and were randomly allocated to the treatment they did not prefer; and patients who had no preference.
Patients who were randomised to their preferred treatment had a standardised effect size greater than that of those who were indifferent to the treatment assignment (effect size 0.162, 95% confidence interval 0.011 to 0.314; P=0.04). Participants who received their preferred treatment also did better than participants who did not receive their preferred treatment (effect size 0.152, -0.035 to 0.339), although this was not statistically significant (P=0.11). Participants allocated to their undesired treatment had outcomes that were no different from those who were indifferent. Participants who were allocated to their undesired treatment were less likely to be lost to first follow-up compared with indifferent participants (odds ratio 1.70, 1.076 to 2.693; P=0.02). No difference was found in attrition between patients allocated to their preference and those who were indifferent.
Preferences among patients in musculoskeletal trials are associated with treatment effects. In open randomised trials, preferences should be ascertained before randomisation.
系统评价完全随机的患者偏好试验,并通过对患者层面数据的荟萃分析探讨偏好对失访和结局的影响。
使用科学引文索引和谷歌学术进行引文检索,并结合关键词检索主要电子数据库(医学索引、护理学与健康领域数据库、荷兰医学文摘数据库和联合和补充医学数据库)。
纳入比较针对任何临床病症的治疗方法的完全随机患者偏好试验。排除其他类型的偏好试验和交叉试验。其他纳入标准:年龄16岁及以上的参与者;以连续数值量表测量的主要的、自我报告的结局。从167项被识别和筛选的研究中,有17项被确定为完全随机患者偏好试验。
在确定的17项试验中,11位作者提供了用于荟萃分析的原始数据。收集的数据包括主要结局的基线和随访数据、随机分配数据、偏好数据和人口统计学数据。主要结局的基线和干预后首次随访数据进行了标准化处理。为提高同质性,仅合并了八项肌肉骨骼试验(n = 1594)的数据。为估计偏好对结局和失访的影响,比较了三组:有偏好并被随机分配到其偏好治疗的患者;有偏好并被随机分配到其不偏好治疗的患者;以及无偏好的患者。
被随机分配到其偏好治疗的患者的标准化效应量大于对治疗分配无差异的患者(效应量0.162,95%置信区间0.011至0.314;P = 0.04)。接受其偏好治疗的参与者也比未接受其偏好治疗的参与者表现更好(效应量0.152,-0.035至0.339),尽管这在统计学上不显著(P = 0.11)。被分配到其不期望治疗的参与者的结局与无差异的参与者无异。与无差异的参与者相比,被分配到其不期望治疗的参与者在首次随访时失访的可能性较小(优势比1.70,1.076至2.693;P = 0.02)。在被分配到其偏好治疗的患者和无差异的患者之间,失访情况未发现差异。
肌肉骨骼试验中患者的偏好与治疗效果相关。在开放随机试验中,应在随机分组前确定偏好。