Grace Clare, Begum Reha, Subhani Syed, Kopelman Peter, Greenhalgh Trisha
Barts and the London School of Medicine and Dentistry, Queen Mary University of London E1 2AT.
BMJ. 2008 Nov 4;337:a1931. doi: 10.1136/bmj.a1931.
To understand lay beliefs and attitudes, religious teachings, and professional perceptions in relation to diabetes prevention in the Bangladeshi community.
Qualitative study (focus groups and semistructured interviews).
Tower Hamlets, a socioeconomically deprived London borough, United Kingdom.
Bangladeshi people without diabetes (phase 1), religious leaders and Islamic scholars (phase 2), and health professionals (phase 3).
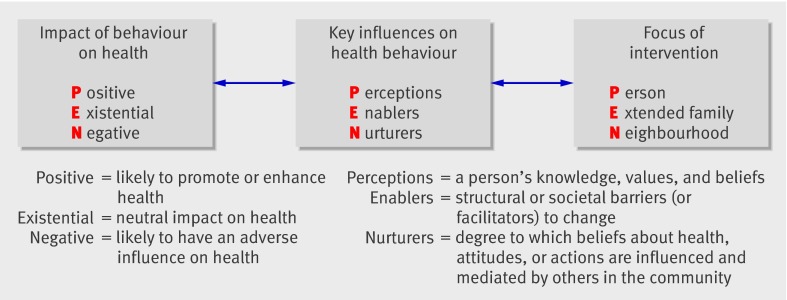
17 focus groups were run using purposive sampling in three sequential phases. Thematic analysis was used iteratively to achieve progressive focusing and to develop theory. To explore tensions in preliminary data fictional vignettes were created, which were discussed by participants in subsequent phases. The PEN-3 multilevel theoretical framework was used to inform data analysis and synthesis.
Most lay participants accepted the concept of diabetes prevention and were more knowledgeable than expected. Practical and structural barriers to a healthy lifestyle were commonly reported. There was a strong desire to comply with cultural norms, particularly those relating to modesty. Religious leaders provided considerable support from Islamic teachings for messages about diabetes prevention. Some clinicians incorrectly perceived Bangladeshis to be poorly informed and fatalistic, although they also expressed concerns about their own limited cultural understanding.
Contrary to the views of health professionals and earlier research, poor knowledge was not the main barrier to healthy lifestyle choices. The norms and expectations of Islam offer many opportunities for supporting diabetes prevention. Interventions designed for the white population, however, need adaptation before they will be meaningful to many Bangladeshis. Religion may have an important part to play in supporting health promotion in this community. The potential for collaborative working between health educators and religious leaders should be explored further and the low cultural understanding of health professionals addressed.
了解孟加拉社区中与糖尿病预防相关的大众观念和态度、宗教教义以及专业认知。
定性研究(焦点小组和半结构化访谈)。
英国伦敦社会经济贫困的陶尔哈姆莱茨区。
无糖尿病的孟加拉人(第一阶段)、宗教领袖和伊斯兰学者(第二阶段)以及健康专业人员(第三阶段)。
采用目的抽样法分三个连续阶段进行了17个焦点小组讨论。反复使用主题分析法以实现逐步聚焦并发展理论。为探究初步数据中的矛盾点,创作了虚构的小插曲,并在后续阶段由参与者进行讨论。使用PEN - 3多层次理论框架为数据分析和综合提供信息。
大多数普通参与者接受糖尿病预防的概念,且比预期更有知识。普遍报告了健康生活方式的实际和结构障碍。人们强烈希望遵守文化规范,尤其是与谦逊相关的规范。宗教领袖从伊斯兰教义中为有关糖尿病预防的信息提供了大量支持。一些临床医生错误地认为孟加拉人了解不足且宿命论,但他们也表达了对自身文化理解有限的担忧。
与健康专业人员的观点和早期研究相反,知识匮乏并非健康生活方式选择的主要障碍。伊斯兰教的规范和期望为支持糖尿病预防提供了许多机会。然而,为白人设计的干预措施在对许多孟加拉人有意义之前需要进行调整。宗教在支持该社区的健康促进方面可能发挥重要作用。应进一步探索健康教育工作者与宗教领袖合作的潜力,并解决健康专业人员文化理解不足的问题。